Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
344 Cards in this Set
- Front
- Back
|
What is TART?
|
Tissue Texture Change
Asymmetry Restriction Tenderness findings of somatic dysfunction |
|
|
a point at which a pt can actively move any given joint. Ex: a person may actively rotat his head80 degrees to either side...this is an example of?
|
Physiological Barrier
|
|
|
Point at which a physician can passively move any joint. Ex: a doc can move a pt head to 90 degrees while the pt can only move 80 on their own
|
Anatomic Barrier
|
|
|
Movement beyond the anatomical barrier results in?
|
ligament, tendon or skeletal injury
|
|
|
compared to midline, where do physiological, anatomic, and pathologic barriers lie?
|
closest to midline: pathologic
then physiologic then anatomic |
|
|
pt can turn their head 80 degrees to the right, physician can turn the pt head 90 degrees each way. The pt can only turn their head 70 degrees to the left... what is going on?
|
Restrictive (pathological) barrier
remember this will always be less than the physiologic |
|
|
What is the only subjective component of TART?
|
Tenderness
|
|
|
For the following tissue texture change, describe if it is acute or chronic:
Edematous erythematous, boggy, with increased moisture. Mucles are hypertonice |
Acute
|
|
|
For the following tissue texture change, describe if it is acute or chronic:
Decrease or no edema, no erythema, cool dry skin with slight tension. Decreased muscle tone, flaccid, ropy, fibrotic |
Chronic
|
|
|
For the following Asymmetry, describe if it is acute or chronic:
Present |
Acute
|
|
|
For the following Asymmetry, describe if it is acute or chronic:
Present with compensation in other areas of the body |
Chronic
|
|
|
For the following restriction, describe if it is acute or chronic:
Present, painful with movement |
Acute
|
|
|
For the following restriction, describe if it is acute or chronic:
Present, decreased or no pain |
chronic
|
|
|
For the following tenderness, describe if it is acute or chronic:
Severe or sharp |
Acute
|
|
|
For the following tenderness, describe if it is acute or chronic:
dull, achy, burning |
chronic
|
|
|
Describe Fryettes law one
give an example are the facets engaged or not? does rotation or side bending come first? |
if the spine is in the neutral position (no flexion or extension) and if sidebending is introduced, rotation would then occur to the opposite side...applies to more than two vertebral segments
Side bending precedes rotation and the occur in opposite directions NSLRR Facets not engaged usually compensatory seen in long curves with multiple segments |
|
|
Describe Fryettes law II
give an example are the facets engaged? does rotation or side bending come first? |
rotation and sidebending occur in the same way
Single vertebral segment Rotation precedes sidebending, and they occur in the same direction Ex: FRRSR Facets are engaged Found at apices and crossovers Single segment |
|
|
Where do Fryettes laws apply?
|
Thoracic and lumbar only
not Cervical |
|
|
What is Law III?
|
initiating motion at any segment in any one plane of motion will modify the mobility of that segment in the other planes of motion
ex: Forward bending will decrease the ability to sidebend and rotate |
|
|
how are somatic dysfunctions named
|
for their freedom of motions
|
|
|
give the somatic dysfunction for:
L2 is restricted in the motions of flexion, sidebending to the right and rotation to the right |
L2 ERLSL
|
|
|
TRIGGER POINT:
what is the superior facet orientation for Cervical, Thoracic, and Lumbar spine? |
Cervical: Backward, upward, medial--->BUM
Thoracic: backward upward lateral-->BUL Lumbar: backward, medial-->BM |
|
|
If doing a direct tx for T3 FRRSR how would the practitioner move the joint?
|
Extend
rotate left Sidebend left |
|
|
TRIGGER POINT
What is the difference in active/passive tx? what about direct/indirect tx? |
Active: pt will assist in the tx, usually in the form of isometric or isotonic contraction
Passive: the pt will relax and allow the doc to move the body tissues Direct: Towards the Barrier Indirect: away from the barrier |
|
|
For the following, list if the tx is direct/indirect/both and if the motion can be active/passive/both:
MFR CS Facilitated postional release ME HVLA Cranial Lymphatic tx Chapmans |
Direct or indirect / Active or Passive
MFR: Both / Both CS: Indirect / Passive Facilitated postional release: Indirect / Passive ME: Direct / Active HVLA: Direct / Passive Cranial: Both / Passive Lymphatic tx: Direct / Passive Chapmans: Direct / Passive |
|
|
Elderly and hospital pts respond better to what kind of techniques?
|
indirect or gentle direct such as articulatory
|
|
|
the use of what kind of tx in a pt with advanced osteoporosis or metastatic dz can lead to a pathologic fracture
|
HVLA
|
|
|
Acute neck strain/sprains are often treated with what kind of techniques to prevent further strain?
|
indirect
|
|
|
discuss how frequently you can tx the following pts with OMT:
Sicker pts Pediatric Acute cases |
Sicker pts: limit to a few key areas
Pediatric: more frequent tx allowed (geriatrics need more time btw tx) Acute cases:shorter interval btw tx (increase frequency) |
|
|
pt has rib problem, upper thoracic spine problem, and cervical spine...which should you tx first?
|
Ribs and upper thoracic before C spine
|
|
|
which do you tx first, thoracic spine or rib?
|
Thoracic spine
|
|
|
for extremity problems, what should you tx first?
|
spine, sacrum and ribs first
(axial skeleton b4 periphery) |
|
|
Patient presents with a positive left standing flexion test. Left ASIS is cephalad. Left PSIS is cephalad. What is pelvic diagnosis?
|
Left superior Innominate Shear
|
|
|
which vertebrae has no spinous processes or vertebral body?
which has a dens? |
no spinous: C1
dens: C2 |
|
|
Patient has positive ASIS compression test
on the left. Both left ASIS and left PSIS are caudad. What is your diagnosis? |
Left inferior innominate shear
|
|
|
What muscle will help elevate the first rib during forced inhalation?
2nd rib? |
1st: anterior/middle scalene
2nd: posterior |
|
|
Positive Standing tests on the left. Positive ASIS compression test on the left. What does this tell you? Left ASIS caudad. Left PSIS cephalad.
What is the diagnosis? |
Left Anterior Innominate rotation
|
|
|
What muscle often has a tender point when the there is 1st or seconds inhalation rib dysfunction?
|
Scalene
|
|
|
Positive Standing test left. Left ASIS is cephalad and left PSIS is caudad
What is the diagnosis? |
Left Posterior Innominate Rotation
|
|
|
motion of the SCM?
|
with unilateral contraction the SCM will sidebend ipsilaterally and rotate contralaterally (Think of cracking your neck)
bilateral contraction will flex the neck |
|
|
Positive ASIS compression test on right. Right ASIS closer to midline relative to left. What is the diagnosis?
|
Right innominate inflare
|
|
|
shortening restrictions within the SCM result in what?
|
torticollis
(twisted neck in which the head is tipped to one side, while the chin is turned to the other) |
|
|
Patient presents with sacroiliac pain. She has a positive seated flexion test on the right. She has a negative spring test. L2-5 are NRRSL. The right sacral base is anterior and the Left ILA is posterior. What is her sacral diagnosis?
|
Seated flexion test positive on Right:
What does this tell you? Right SI joint is restricted and has Left oblique axis if engaged Negative spring test: What does this tell you? L/S junction can flex, ie forward rotation L5 rotated right: Sacrum rotates left L5 sidebent left: Left oblique axis Right base anterior Left ILA posterior What is your diagnosis? Left on Left Sacral Torsion |
|
|
Positive ASIS compression test left. Left ASIS further from midline relative to right. What is your diagnosis?
|
Left innominate outflare
|
|
|
Seated flexion test positive on left. Negative backward bending test (findings become more symmetrical). L3-5 are NRLSR. Assuming physiologic motion between lumbar and sacrum, can you give diagnosis?
|
Seated flexion test positive on left:
What does this tell you? Left SI joint is restricted and has Right oblique axis if engaged Negative backward bending test (findings become less asymmetrical): What does this tell you? sacrum can flex (ie forward torsion) L5 rotated Left: Sacral rotation right L5 is sidebent to right Right oblique axis Left base would be anterior Right ILA would be posterior What is your diagnosis? Right on Right Sacral torsion |
|
|
Rheumatoid arthritis and down's syndrome can weaken what ligaments and lead to A-A subluxation?
|
alar (dens to foramen magnum)
transverse (attaches dens to lateral masses of C1 to hold dens into place) |
|
|
Seated flexion test positive on right with positive spring test. L5 is rotated left. The right sacral base is posterior and the Left ILA anterior. What is the diagnosis?
|
Seated flexion test positive on Right
What does that tell you? Left sacral axis Positive spring test What does that tell you? L/S junction is extended (can’t flex) backward torsion L5 rotated left: What does that tell you? sacral rotation right on oblique axis Right base posterior Left ILA anterior What is the diagnosis? Right on left torsion |
|
|
What are the Joints of Luschka
|
C3-C7
uncinate process and superadjacent vertebrae play a major role in sidebending degenerative change can lead to foraminal stenosis and nerve root impigment |
|
|
Seated flexion test positive on left with positive spring test. L5 is FRSL. Assuming normal mechanics, what is the sacral diagnosis?
|
Seated flexion test positive on Left
What does that tell you? Right sacral axis Positive spring test What does that tell you? L/S junction is extended (can’t flex) backward torsion L5 rotated right: sacral rotation left L5 sidebent right: Right oblique axis What is the diagnosis? Left on Right torsion |
|
|
what is the most common cause of cervical nerve root pressure?
|
degeneration of the joints of Luschka plus hypertrophic arthritis of the IV joints
|
|
|
Seated flexion/ASIS compression test positive on Left.
Negative Backward Bending Test (findings become less asymmetrical) Left base is anterior and left ILA is posterior and inferior. What is your diagnosis? |
Seated flexion/ASIS compression test positive on Left
What does that tell you? Left SI restriction Negative Backward Bending Test (findings become more symmetrical) What does that tell you? Sacrum prefers flexion Left base is anterior Left ILA posterior and inferior What does this tell you? Not a torsion What is your diagnosis? Left Unilateral Sacral Flexion |
|
|
how do cervical nerves exit?
|
ABOVE their corresponding vertebrae
thus their are 8 so C7 will be btw C6-C7 |
|
|
tx for Left on Left Sacral Torsion (forward)
|
Forward Torsion Muscle Energy
Pt lying on the axis side with the chest down on the table; Flex the knees and hips until motion is felt at the lumbosacral junction, usually at least 90° hip flexion; Allow the legs to hang down off the table with thighs supported by your leg Monitor the anterior sacral base and ask the patient to push the feet toward the ceiling for 3-5 seconds against your equal resistance; Slowly move the legs toward the floor to a new restrictive barrier; Repeat 3-5 times or until return of sacral mobility; Retest sacroiliac motion or sacral symmetry. |
|
|
why does dmg to the lower cervical cord cause problems in the upper extremity
|
C5-T1 = brachial plexus
|
|
|
tx for Left on Right torsion
|
Backward Torsion Muscle Energy
Technique (lateral recumbent): Sit or stand in front of the patient who is lying on the axis side with the upper back on the table; Extend the leg on the table until motion is felt at the lumbosacral junction; Flex the top leg and place the foot behind the other knee; Hold the shoulder to prevent the patient from rolling and allow the flexed knee to hang down off the table; Ask the patient to push the flexed knee toward the ceiling for 3-5 seconds against your equal resistance; Slowly move the knee toward the floor to a new restrictive barrier; Repeat 3-5 times or until sacral mobility returns; Retest sacroiliac motion or sacral symmetry. |
|
|
What makes up the OA? what is its primary motion(s). How do sidebending and roation occur here?
|
motion of the occipital condyles on the atlas (C1)
flexion and extension sidebending and rotation occur to OPPOSITE sides FRRSL |
|
|
tx for Right Unilateral Sacral Flexion
|
Stand facing the patient’s head on the side of the unilateral flexion;
place your thenar or hypothenar eminence on the involved inferior lateral angle and push it anteriorly and superiorly by leaning into it; Use your other hand to slightly abduct and internally rotate the lower extremity on the involved side; While the patient takes a deep breath, push the sacrum into extension during inhalation and resist sacral flexion during exhalation; Repeat 3-5 times or until sacral mobility returns; Retest sacroiliac motion or sacral symmetry. |
|
|
What makes up the AA? Primary motion?
|
C1 motion on C2
ROTATION clinically only moves in rotation here |
|
|
Seated flexion test positive on left with positive spring test. L5 is FRSR. Assuming normal mechanics, what is the sacral diagnosis?
|
Seated flexion test positive on Left
What does that tell you? Right sacral axis Positive spring test What does that tell you? L/S junction is extended (can’t flex) backward torsion L5 rotated right: sacral rotation left L5 sidebent right: Right oblique axis What is the diagnosis? Left on Right torsion |
|
|
how do C2-C7 move?
|
Sidebending and rotation occur in the same way
NO MATTER THE TYPE SARA CERVICAL (sidebend away, rotate away) |
|
|
Seated flexion/ASIS compression test positive on Left.
Negative Backward Bending Test (findings become less asymmetrical) Left base is anterior and left ILA is posterior and inferior. What is your diagnosis? |
Seated flexion/ASIS compression test positive on Left
What does that tell you? Left SI restriction Negative Backward Bending Test (findings become more symmetrical) What does that tell you? Sacrum prefers flexion Left base is anterior Left ILA posterior and inferior What does this tell you? Not a torsion What is your diagnosis? Left Unilateral Sacral Flexion |
|
|
TRIGGER POINT
For the following segments, describe the main motion and how sidebending and rotation occur with respect to each other: OA: AA: C2-4 C5-7 |
OA: Flexion and Extension / opposite sides
AA: Rotation C2-4: Rotation / Same Sides C5-7: Side bending / Same Sides |
|
|
Seated flexion/ASIS compression
test positive on Left. Positive Spring test. Left base posterior (or right anterior) and Left ILA anterior (or right posterior). What is your diagnosis? |
Seated flexion/ASIS compression
test positive on Left: What does that tell you? Left SI restriction Positive Spring test: What does this tell you? L/S junction is extended (can’t flex) Left base posterior (or right anterior) Left ILA anterior (or right posterior) What is your diagnosis? Left unilateral sacral extension |
|
|
if you translate the OA to the right and it is restricted, what does this tell you?
|
it is restricted in left sidebending
(and thus in R rotation) |
|
|
tx for unilateral sacral extension?
|
Stand facing the patient’s feet on the side of the unilateral extension;
Place your thenar or hypothenar eminence on the involved sacral base, and push it anteriorly and inferiorly by leaning into it; Use your other hand to slightly abduct and internally rotate the lower extremity on the involved side. While the patient takes a deep breath, resist sacral extension during inhalation and push the sacrum into flexion during exhalation; Repeat 3-5 times or until sacral mobility returns; Retest sacroiliac motion or sacral symmetry. |
|
|
when you test AA motion, why do you flex the neck to 45 degrees?
|
remember you are testing rotation here
flexing to 45 degrees will lock out rotation of C2-C7 |
|
|
suboccipital or paravertebral muscle spasms are usually associated with what?
|
upper thoracic or rib problems on the same side
tx these first |
|
|
There is a rule of threes for where the spinous processes are located... so where are they for
T1-T3: T4-6: T7-9: T10 T11 T12: |
T1-T3: located at the level of the corresponding transverse process
T4-6: one half a segment below (spinous process of T5 is halfway btw T5/6) T7-9: Spinous process located at the lvl of the transverse process of the vertebrae below (T8's is at T9) T10: Spinous process located at the lvl of the transverse process of the vertebrae below T11:one half a segment below T12: at the level of T12 transverse process |
|
|
Spine of scapula is where?
inferior angle of scapula= sternal notch= nipple= umbillicus= |
Spine of scapula is where= T3
inferior angle of scapula=T7 sternal notch=T2 nipple= dermatome of T4 umbillicus= dermatome of T10 |
|
|
TRIGGER POINT:
main motion of thoracic spine? |
ROTATION
upper and middle thoracic: rotation >flexion/extension>sidebending lower thoracic: flexion/extension>sidebending>rotation |
|
|
innervation of the diaphragm?
|
Phrenic nerve (C3,4 5, keep the diaphragm alive)
remember the diaphragm also returns lymph and venous blood back to the thorax |
|
|
where do the tubercle and head of a rib articulate respectively?
|
tubercle: corresponding transverse process
head: vertebrae above the corresponding vertebrae and its own |
|
|
what are the atypical ribs?
|
They have "1s" and "2s"
1: atypical because it articulates with only T1 and ha no angle 2: has a large tuberosity on shaft for serratus anterior 11: articulate only with corresponding vertebrae and lack tubercles 12 : same as above (sometimes rib 10: because it articulates only with T10) |
|
|
Trigger point:
What are the differences btw TRUE, FLOATING, and FALSE ribs what rib set are each of these? |
Ribs 1-7: Attach to sternum through costal cartilages-->TRUE
Ribs 8-12: do not attach directly to sternum (each is connected by its costal cartilage to the cartilage above)-->FALSE Ribs 11-12: remain unattached anteriorly-->FLOATING |
|
|
which ribs move by pump handle, bucket handle, and caliper handle
|
Pump: 1-5
Bucket: 6-10 Caliper: 11-12 |
|
|
what is an inhalation dysfunction?
|
exhalation dysfunction
dysfunctional rib will move cephalad druing inhalation however: the dysfunctional rib will not move caudad during exhalation rib appears to be held up |
|
|
is this an inhalation or exhalation rib? pump handle or bucket handle?
rib elevated anteriorly anterior part of rib moves cephalad on inspiration and restricted on expiration anterior narrowing of intercostal space above the dysfunctional rib superior edge of posterior rib angle is promienent (sublexed) |
Pump handle (1-5)
inhalation SD |
|
|
is this an inhalation or exhalation rib? pump handle or bucket handle?
rib elevated laterally lateral part (shaft) of rib moves slightly upward on inspiration and restricted on expiration lateral narrowing of intercostal space above dysfunctional rib lower edge of rib shaft is prominent |
Bucket Handle (6-10)
inhalation SD |
|
|
is this an inhalation or exhalation rib? pump handle or bucket handle?
rib depressed anteriorly ant part of rib moves caudad on expiration and restricted on inspiration anterior narrowing of intercostal space below dysfunctional rib inferior edge of posterior rib angle is prominent |
pump handle (1-5)
exhalation SD |
|
|
is this an inhalation or exhalation rib? pump handle or bucket handle?
rib depressed laterally lateral part (shaft) of rib moves slightly downpward on expiration and restricted on inspiration lateral narrowing of intercostal space below dysfunctional rib |
bucket handle ribs (6-10)
exhalation SD |
|
|
in inhalation and exhalation dysfunctions what is the key rib
|
key rib is the troublemaker
inhalation: lowest rib exhalation: upper rib |
|
|
pt has exhalation rib dysfunction from rib 2-5, which do you tx?
|
rib 2
|
|
|
what ligament narrows in the lumbar region (at L4 is is half the width of it was at L1)...? What does this lead to?
|
Posterior longitudinal ligament
more susceptible to disc herniation |
|
|
in the thoracic and lumbar region, how do nerve roots exit the IV foramen?
|
BELOW
L4 nerve root will come out btw L4 and L5 |
|
|
where does the spinal cord terminate?
|
L1/2
|
|
|
What is the primary flexor of the hip?
|
Iliopsoas
Origin: T12-L5 vertebral bodies |
|
|
what makes up the erector spinae group?
|
I Love Spaghetti
Iliocostalis Longissimus Spinalis |
|
|
pelvic side shift, positive Thomas Test (checks for exaggerated lumbar lordosis + flexion of hip), and SD of an upper lumbar segment are commonly seen with what?
|
Iliopsoas SD
|
|
|
what landmark is at the iliac crest
|
L4-5 IV disc
|
|
|
TRIGGER POINT
What are the 3 types of spina bifida |
Defect in closure of lamina of vertebral segment
Occulta: no herniation through defect, only sigh is normally a patch of hair meningocele: herniation of meninges meningomyelocele: meninges and nerve roots herniate (assoc with neurological defects) |
|
|
TRIGGER POINT:
Major motion of the lumbar spine? |
Flexion extension
(remember for thoracic it was rotation) |
|
|
rotation of the L5 will cause what to happen to the sacrum?
|
it will be rotated toward the opposite side
|
|
|
What is the Lumbosacral (Ferguson's) angle?
does an increase or decrease in angle cause back pain? |
formed by intersection of a horizontal line and the line of the inclination of the sacrum
usually btw 25-35 degrees increase in angle causes shear stress and causes low back pain |
|
|
Where do 90% of herniated discs occur?
|
between L4 and L5
or L5 and S1 |
|
|
Herniation btw L3 and L4 will affect what nerve?
what movement would make it worse? |
L4
flexion- moves the pulposis further posterior |
|
|
how can you diagnose a herniated disc?
|
straight leg test
|
|
|
tender point medial to the ASIS, nonneutral dysfunction of L1 or L2, and pelvic shift test to the contralateral side can be signs of what?
|
Psoas syndrome
can also be due to sacral dysfunction on an oblique axis and contralateral periformis spasm note: that for tx, you should get rid of the high lumbar strain first |
|
|
TRIGGER POINT:
A flexion contracture of the iliopsoas is often associated with what? |
a nonneutral dysfunction of L1 or L2
|
|
|
TRIGGER POINT:
What is spondylolisthesis? what is a spondylolysis? Spondylosis? |
spondylolisthesis: Anterior displacement of one vertebrae in relation to the one below
Spondylolysis: defect of the pars interarticularis WITHOUT anterior displacement. Oblique view will show a fracture of the pars (seen as the collar of the scotty dog) Spondylosis: Degenerative changes within the IV disc and anklosing of adjacent vertebral bodies |
|
|
pt comes to your office complaining of low back pain. They have tight hamstrings, stiffed legged short stride waddling gait. You palpate and feel a positive vertebral step off sign and the pain is increased with extension. What does this pt have?
|
Spndylolisthesis
positive vertebral step-off sing= palpating the spinous processes there is an obvious forward displacement at the area of listhesis |
|
|
TRIGGER POINT:
What view on X ray do you use to diagnose a spondylolisthesis? what about a spondylolysis? what where these again? |
LATERAL XRAY: spondylolisthesis: Anterior displacement of one vertebrae in relation to the one below
OBLIQUE XRAY Spondylolysis: defect of the pars interarticularis WITHOUT anterior displacement. Oblique view will show a fracture of the pars (seen as the collar of the scotty dog) |
|
|
pt comes in with saddle anesthesia, decreased DTRs, decreased recal sphincter tone leading to loss of bowel and actually bladder control as well...what does he have? Cause? tx?
|
Cauda Equina syndrome
usually due to massive central disc herniation (or use of local anesthetics) tx: emergent surgical decompression of the cauda equina is imperitive, if surgery is delayed too long paralysis may result |
|
|
What is a dextroscoliosis?
Levoscoliosis? |
curve that is sidebending left = scoliosis to the right = dextroscolisosis
curve that is sidebent right = socliosis to the left = levoscoliososis |
|
|
What is the difference btw a structural and functional curve?
|
Structural: fixed and inflexible, will not correct
Functional: flexible that is partially or completely corrected with sidebending to the opposite side (uncorrected may become structural) |
|
|
when evaluating for scoliosis, you examine the levelness of the occiput, shoulders, iliac crests, PSIS and greater trochanters. If these are not level, what should you check next?
|
have the pt bend forward, if a group of ribs appear higher on one side as the pt bends forward (rib hump) the pt is likely to have scoliosis
|
|
|
What is the Cobb angle
What does 5-15 show? What about beyond that? |
shows scoliosis
draw horizontal line from the vertebral body of the extreme ends of the curve, then perpendicular lines off the previous 2 5-15: mild scoliosis 20-45: moderate >50: Severe |
|
|
at what Cobb angles do you see respiratory functioning compromised and CV function compromised respectively?
|
Resp: >50
CV: >75 |
|
|
What are the tx for the following scoliosis:
Mild Moderate Severe |
5-15: mild scoliosis
--OMT and Konstancin exercises 20-45: moderate --above + bracing + spinal orthotic >50: Severe --Surgery if resp compromise |
|
|
most common cause of anatomical short leg?
|
hip replacement
|
|
|
describe if the following findings will be on the side of the short or the long leg in a person with short leg syndrome:
1. sacral base lower 2. ant inominate roatoin 3. post inominate rotation 4. Lumbar will side bend away and rotate toward the side of the.. 5. Iliolumbar followed by the SI ligaments will become stressed on the side of... |
1. short leg
2. short leg 3. long leg 4. short leg 5. short leg |
|
|
if the difference btw the heights of the femoral head is ____ you should use a ____ ____ for tx
|
>5mm
Heel lift |
|
|
in a fragile pt (elderly, arthritic, osteoporotic, or those in acute pain) you should begin with what size heel lift? How should you increase it?
|
1/16" (1.5mm)
increase 1/16" every 2 weeks |
|
|
in a flexible pt, you should begin with what size heel lift? how should you increase it from there?
|
1/8" (3.2mm)
1/8" every 2 weeks |
|
|
maximum inches heel lift you can add to the inside of the shoe? max total?
|
inside: 1/4" (rest must be added outside)
total: 1/2" note: final lift should be 1/2 -3/4" original discrepancy |
|
|
TRIGGER POINT:
What divides the greater and lesser sciatic foramen? |
The sacrospinous ligament
originates at the sacrum and attaches to the ischial spines |
|
|
what 2 muscles make up the pelvic diaphragm?
|
levator ani
coccygeus muscle |
|
|
11% of the population will have either the entire or peroneal portion of the sciatic nerve running through the belly of what muscle? Where can this cause pain? Radiating to?
|
Piriformis
Buttock pain that radiates down the thigh but not below the knee |
|
|
How does the sacral base move in respiratory motion
|
Inhalation-->spine elongates-->sacral base posterior
Exhalation: anterior |
|
|
how will the sacrum move in inherent (craniosacral) motion? (how does the base move in craniosacral flexion/extension)
|
during craniosacral flexion: posterior (counternutates)
during extension: anteriorly (nutates-nods forward) remember: cranial flexion=fat head extension= thin head |
|
|
TRIGGER POINT:
What are the axes of the sacrum? |
DRIP
Dynamic (weight bearing engages sacral axis) Respiratory (inhale-base goes posterior) Inherent (cranial): flexion-base goes posterior/counternutates Postural- as person bends forward sacral base goes anterior |
|
|
ASIS inferior
PSIS superior same side and positive standing flexion test on that side |
Anterior inominate rotation
will have longer leg ipsilaterally |
|
|
common etiology of the following:
asis and psis move superiorly ipsilaterally |
This is a superior inominate sheer
Due to a fall |
|
|
common etiology of the following:
ASIS more superior ipsilaterally PSIS more inferior ipsilaterally |
this is a posterior inominate rotation
due to tight hamstrings |
|
|
common etiology of the following:
ASIS's level PSIS's level Pubic bone superior ipsilaterally |
this is a superior pubic shear
due to trauma or tight rectus abdominus muscle |
|
|
common etiology of the following:
ASIS's level PSIS's level Pubic bone inferior ipsilaterally |
this is a inferior pubic shear
due to trauma or tight aDductors |
|
|
TRIGGER POINT:
Sacral Torsion rules: 1. When L5 is sidebent, a sacral oblique axis is engaged on the ____ side as the sidebending 2. When L5 is rotated, the sacrum rotates ____ on an oblique axis 3. The seated flexion test is found on the ___ side of the oblique axis |
1. When L5 is sidebent, a sacral oblique axis is engaged on the _SAME_ side as the sidebending
2. When L5 is rotated, the sacrum rotates _THE OPPOSITE WAY_ on an oblique axis 3. The seated flexion test is found on the _OPPOSITE_ side of the oblique axis |
|
|
If L5 is FRRSR
where will the seated flexion test be positive? how will the sacrum be rotated? |
Positive seated flexion on the LEFT
The sacrum will be rotated to the left on a right oblique axis...or L on R |
|
|
In sacral torsions, L5 will always rotate in the ____ direction of the sacrum
|
OPPOSITE
|
|
|
What is a positive spring test? what does it show?
|
Resistance to springing
Sacral extension (posterior) Backward torsion (R on L or L on R) |
|
|
What is a negative spring test? what does it show?
|
Ease of springing
Sacral flexion Forward torsion (R on R or L on L) |
|
|
How do a sacral rotation and sacral torsion differ?
--this seems to me to be low yield |
Rotation: L5 and sacrum rotate to same way
Torsion: rotate in opposite side |
|
|
Findings:
RIght and left sulci (sacral base) deep ILA's shallow bilaterally FALSE negative seated flexion test negative lumbosacral spring test Diagnosis? |
Bilateral sacral flexion
the entire sacral base moves anterior about a middle transverse axis |
|
|
TRIGGER POINT:
Bilateral sacral flexion is a common dysfunction in what type of pt? |
Post-partum
remember: Findings: RIght and left sulci (sacral base) deep ILA's shallow bilaterally FALSE negative seated flexion test negative lumbosacral spring test |
|
|
Findings:
RIght and left sulci (sacral base) shallow ILA's deep bilaterally FALSE negative seated flexion test positive lumbosacral spring test |
Bilateral Sacral Extension
|
|
|
Left sulcus deeper
Left ILA significantly inferior left ILA slightly posterior Positive seated flexion on the left motion (springing) at the left sulcus is present diagnosis? |
Left unilateral sacral flexion
|
|
|
Right sulcus shallow
Right ILA anterior Positive seated flexion on the right Positive lumbosacral spring test Diagnosis? |
right unilateral sacral extension
|
|
|
pt has lumbar and sacral problems..which do you tx first?
|
LUMBAR
so treat L5 first! most sacral problems disappear with this |
|
|
if a person has a flexion contracture of the iliopsoas on the the right, what other findings could you expect to see?
|
L1 or L2 may be FRRSR
|
|
|
What is the only bone connecting the upper extremity and the axial spine?
|
Clavicle
|
|
|
TRIGGER POINT:
What are the rotator cuff muscles and their actions? |
SItS
Supraspinatous: abduction of arm Infraspinatus: external rotation of the arm Teres Minor: external rotation of the arm Subscapularus: internal rotation of the arm |
|
|
Muscles of the shoulder...given the action list the muscle:
Primary flexor: Primary abductor: Primary extensors: Primary adductors: Primary external rotators: Primary internal rotator: |
Primary flexor: Deltoid
Primary abductor: Deltoid Primary extensors: Lat dorsi, teres major, deltoid Primary adductors: pec major, lat dorsi Primary external rotators: infraspinatus, teres major Primary internal rotator: subscapularis |
|
|
given the radial and ulnar arteries, which supplies the deep palmar and superficial palmar arteries?
|
radial: deep palmalr
ulnar: superficial |
|
|
tx for relieving lymph congestion of the upper extremity?
|
open the thoracic inlet
redome the thoracoabdominal diaphragm posterior axillary fold technique (?? no idea what this is) |
|
|
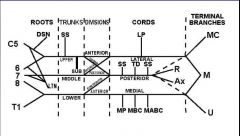
Draw the Brachial Plexus
|
|
|
|
normally the arm can abduct to 180 with active motion...120 is due to glenohumeral motion and 60 is due to scapulothoracic motion. There for for every 3 degrees of abduction, the glenohumeral joint moves __ degrees and the scapulothoracic joint moves __ degrees
|
for for every 3 degrees of abduction, the glenohumeral joint moves _2_ degrees and the scapulothoracic joint moves _1_ degrees
|
|
|
describe the Spencer Technique
|
Extension
Flexion Compression Traction Abduction Internal Rotation Pump EVERY FAT CAT TRIES ABDUCTING IN PUMPS |
|
|
Most common SD of the shoulder is in what 2 movements? what muscles are responsible?
|
Internal rotation: subscap
External rotation: infraspinatous and teres minor |
|
|
each end of the clavicle can glide... what are its motions?
|
anterior or posterior
OR superior or inferior note: motions at either end of the clavicle are in opposite directions (lateral end of clavicle is superior, medial end is inferior) |
|
|
most common sternoclavicular joint SD?
|
clavicle is anterior and superior on the sternum
clavicle resists posterior and inferior glide |
|
|
What is Thoracic outlet syndrome? What 3 places can this problem occur?
|
Compression of the neurovascular bundle (subclavian artery and vein and the brachial plexus) as it exits the thoracic outlet
Three Places: 1. btw the anterior and middle scalenes 2. Btw the clavicle and 1st rib 3. Btw pec minor and upper ribs |
|
|
pt presents with a positive Adson's test...what is this? what would this show?
What is a Military posture test going to show you? Hyperextension? |
All can show you the location of Thoracic outlet syndrome
Adson's: if compression btw scalenes Military: if compression is btw clavicle and 1st rib Hyperextension: if compression occurs under pectoralis minor |
|
|
Tx for thoracic outlet syndrome should be targeted where?
|
OMT at C2-C7
T1 Rib 1 Thoracic inlet Clavicle Scalenes |
|
|
pain at the tip of the acromion that is exacerbated by abduction especially from 60-120 degrees
|
Supraspinatous tendinitis
|
|
|
Pt comes in complaining of shoulder pain. You find a tenderpoint just below the tip of the acromion and see weakness in active abduction. What special test should you apply?
|
Drop arm test (empty can would probably be good too)
this is a rotator cuff tear, likely in the supraspinatous |
|
|
pt comes in complaining of pain in their shoulder and difficulty moving it. You note decreased ROM with active and passive motion. What is the etiology of this problem? OMT Tx?
|
this is Adhesive capsulitis/ Frozen shoulder syndrome
Etiology: prolonged immobility of the shoulder Tx: main is prevention, but the SPENCER technique is good for improving motion and lysing adhesions |
|
|
You are a sideline doc at a Red Wings game. Kronwall absolutely wrecks Sidney Crosby and it looks like he has a dislocated shoulder. How will the shoulder likely be dislocated? What muscle strength should you make sure to check and why?
|
Anteriorly and inferiorly
Check abduction (deltoid) because the axillary nerve can be damaged |
|
|
Person has a winged scapula...what nerves are involved? muscles?
|
Long thoracic n.
Anterior serratus muscle |
|
|
TRIGGER POINT:
What is the most common type of brachial plexus injury? cause? |
Erb-Duchenne's palsy
upper arm paralysis caused by injury to C5 and C6 nerve roots, usually during child birth (or falling on your shoulder and outstretched neck) |
|
|
What is Klumpke's palsy
|
due to C8-T1 injury
leads to paralysis of the intrinsic muscle of the hand (total claw hand) |
|
|
A man is on crutches for a long time and now is complaining that he his wrist is just flopping around...what does he have? cause?
|
Crutch palsy
compression of the radial nerve |
|
|
Hand bones?
|
Scaphoid
Lunate Triquetral Pisiform Trapezium Trapezoid Hamate capitate |
|
|
nerve that is responsible for:
flexion of the wrist and hand |
median
|
|
|
nerve that is responsible for:
extension of the wrist and hand |
radial
|
|
|
nerve that is responsible for:
supination |
biceps-->musculocutaneous n.
supinator-->radial |
|
|
nerve that is responsible for:
pronation |
median
|
|
|
where do the flexor digitorum profundus and the flexor digitorum superficialis attach respectively?
|
profundus: Distal interphalengeal joint (DIP)
superficialis: PIP |
|
|
what will the carrying angle be for abduction and adduction of the ulna SD?
|
abduction: carrying angle >15
adduction: <3 |
|
|
TRIGGER POINT
An increase in the carrying angle will do what to the ulna (abduct or adduct?) what will this cause in the wrist? |
Increased carrying angle-->abduction of the ulna-->Adduction of the wrist
note the converse is also true |
|
|
how will the radial head glide in pronation and supination respectively?
|
Pronation: posterior
Supination: anterior |
|
|
A man falls forward on an outstretched arm.. what would you likely find his radial head to be like? what restrictions would he have?
|
Posterior radial head
Restriction supination restricted ant glide |
|
|
Man falls backward on to his arm...what would you likely find his radial head to be like? what restrictions would he have?
|
Anterior radial head
restricted in pronation and posterior glide |
|
|
pt comes in complaining of pareshesia on the thumb and first 2 digits, including half of their ring finger. What do they have? Cause? Special Tests?
|
Carpal Tunnel
Entrapment of the median nerve at the wrist Tinel's, Phalen, prayer test tx: rib/upper thoracid SD to decrease sympathetic tone cervical SD to enhance brachial plexus Direct MFR to wrist |
|
|
A man comes in complaining of elbow pain after a long tennis match. What does he have?
|
Lateral epicondylitis (tennis elbow)
pain over lateral epicondyle that worsens with wrist extension |
|
|
Pathogenesis of golfer's elbow?
|
this is medial epicondylitits
due to overuse of the forearm flexors and pronators |
|
|
What is a Swan-neck deformity? Assoc with?
|
flexion contracture of MCP and DIP
extension contracture of the PIP assoc with RA |
|
|
What is a Boutonniere deformity?
assoc with? |
Extension contracture of the MCP and DIP
Flexion contracture of the PIP RA |
|
|
Describe:
Claw Hand Ape Hand Bishops Deformity |
Claw Hand: extension of the MCP, flexion of the PIP and DIP-->results from median and ulnar injury
Ape Hand: Similar to claw, but wasting of the thenar eminence and thumb is adducted-->due to median n. dmg Bishops Deformity: Contracture of the last 2 digits with atrophy of the hypothenar eminence due to ulnar n. dmg |
|
|
How does the head of the femur glide with external and internal rotation respectively?
|
External: anterior
internal: posterior |
|
|
pt has a hip that is restricted in internal rotation....SD? Etiology?
pt has a hip that is restricted in external rotation....SD? Etiology? |
restricted in internal rotation-->External rotation SD-->Piriformis or Iliopsoas spasm
restricted in external rotation-->internal rotation SD-->spasm of internal rotators (gluteus minimus, semimembranous, semitendinous, etc) |
|
|
origin/insertion of the ACL...function?
|
originates at posterior aspect of the femur
attaches to the anterior aspect of the tibia prevents anterior translation of the tibia on the femur |
|
|
origin/insertion of the PCL...function?
|
originates on the anterior aspect of the femur and inserts on the posterior aspect of the tibia.
Prevents posterior translation of the tibia on the femur |
|
|
How will the fibular head move with pronation and supination of the foot respectively?
|
pronation: fibular head moves anterior
supination: fibular head moves posterior note: Dorsiflexion, eversion and abduction=pronation of the anke Plantarflexion, inversion, adduction= supination of the anke |
|
|
TRIGGER POINT
Dorsiflexion, eversion and abduction= _____ of the anke Plantarflexion, inversion, adduction= _____ of the |
Dorsiflexion, eversion and abduction=pronation of the anke
Plantarflexion, inversion, adduction= supination of the |
|
|
person has problem extending their knee, what nerve is dmged? spinal levels?
|
femoral L2-4
|
|
|
Spinal levels for sciatic verve
|
L4-S3
|
|
|
the normal angle between the neck and shaft of the femur is 120-135
What is coxa vara and coxa valga |
coxa vara: <120
Valga: >135 |
|
|
What are Genu Valgum and Varum
make sure you discuss Q angle |
The Q angle is formed by the intersection of a line from the ASIS through the middle of the patella and a line from the tibial tubercle through the middle of the patella. Normally is is 10-12 degrees
an Increased Q angle is referred to GENU VALGUM: knocked kneed A decreased Q angle is genu varum: BOWLEGGED |
|
|
pt has a talus that is internally rotated causing the foot to invert and plantar flex.. what is your diagnosis
anterior fibular head posterior fibular head genu valgum genu varum |
remember: inversion=plantar flex=supination
Posterior Fibular head other findings: proximal fibular head resists anterior spring, distal fibula may be anterior and resist posterior spring |
|
|
pt presents witha proximal fibular head that resists posterior spring... what does the pt have:
anterior fibular head posterior fibular head genu valgum genu varum |
anterior fibular head
could also see: talus externally rotated causing foot to evert and dorsiflex |
|
|
TRIGGER POINT:
What nerve lies directly posterior to the Proximal Fibular head. Therefor a posterior fibular head or fracture of the fibula may disturb the function of this nerve |
Common peroneal (common fibular)
|
|
|
describe a 1-3 degree sprain
|
1st: no tear resulting in good tensile strength and no laxity
2nd: partial tear resulting in a decreased tensile strength with mild to moderate laxity 3rd: complete tear resulting in no tensile strength with mild to moderate laxity (may require surgery) |
|
|
A patient comes to you with severe unrelenting pain. They say it started after working out. You feel the leg and it is rock hard. Which compartment of the leg is most likely to get compartment syndrome?
|
Anterior (ant tibialis muscle is hard and tender to palpation)
note: the lower leg is divided into anterior, lateral, deep posterior, and superficial posterior |
|
|
TRIGGER POINT:
What is the O'Donahue's triad (terrible triad) note: this varies from what first aid 2011 says |
according to green book:
ACL, MCL, Medial Meniscus (FA 2011 says Lateral meniscus) |
|
|
TRIGGER POINT
Is the ankle more stable in dorsi or plantar flexion? Why |
Dorsiflexion
the trochlea of the talus is wider anteriorly, making the foot more stable in dorsiflexion 80% of ankle sprains occur in plantar flexion! |
|
|
Which arch of the foot will be most likely to have SD? What makes up this arch? What type of pt will have this?
|
Transverse arch
Cubiod, Navicular, Cuneiforms Long Distance runners |
|
|
TRIGGER POINT:
What is the most common injured ligament in the foot? |
ATF: Anterior Talofibular ligament
ALWAYS TEARS FIRST |
|
|
What are the 3 types of sprains in the ankle?
|
I: involves anterior talofibular
II: involves ATF and calcaneofibular ligament III: ATF, CFL, and posterior talofibular ligaments all damaged |
|
|
What ligament of the ankle is the medial stabilizer, preventing excessive pronation?
|
Deltoid ligament
excessive pronation will usually result in a fracture of the medial malleoulus rather than a pure ligamentous injury |
|
|
chronic irritation to this structure may cause calcium to be laid down along the lines of stress, leading to a heel spur
|
plantar aponeurosis (fascia)
|
|
|
What is Patello-femoral syndrome? (aka lateral patello-femoral tracking syndrome)
signs/sx? prevalence? tx? |
imbalance of the musculature of the quads (strong vastus lateralis and weak vastus medialis)
deep knee pain especially when climbing stairs more common in women strengthen the vastus medialis muscle |
|
|
TRIGGER POINT
What is the primary respiratory mechanism (PRM) |
CNS + CSF + Dural membranes + cranial bones + sacrum
|
|
|
What is normal Cranial Rhythmic Impulse (CRI)?
|
10-14 cycles per minute
|
|
|
What will effect will the following factors have on CRI (rate/quality):
Stress (emotional/physical) Depression Chronic Fatigue Chronic Infections |
Decrease the rate/quality
|
|
|
What will effect will the following factors have on CRI (rate/quality):
Vigorous physical exercise Systemic Fever Following OMT to the crainosacral mechanism |
Increase the rate/quality
|
|
|
TRIGGER POINT:
What are the Dura Matter's attachments |
Foramen Magnum, C2, C3, S2
|
|
|
What is the reciprocal tension membrane (RTM)
|
connection of dura to the cranial bones, making them move
|
|
|
During flexion, how do the paired bones of the cranium move?
what about during extension? |
flexion: external rotation of paired bones
extension: internal rotation |
|
|
During Fexion of the SBS, how does the pelvis move?
|
dura will be pulled cephalad, moving the sacral base:
POSTERIOR (sacral extension or COUNTERNUTATION) |
|
|
widening the head slightly and decreasing its anterioposterior diameter =
|
cranial flexion
|
|
|
TRIGGER POINT
Craniosacral Flexion: 1. Flexion of the ____ bones 2. Sacral base _____ (_____) 3. ___ AP diameter of the cranium 4. _____ rotation of the paired bones Also, is the movement of the sacrum equivalent to inhalation or exhalation? |
Craniosacral Flexion:
1. Flexion of the _midline_ bones 2. Sacral base _Posterior_ (_Counternutation_) 3. _Decreased_ AP diameter of the cranium 4. _External_ rotation of the pair bones Also, is the movement of the sacrum equivalent to inhalation or exhalation? INHALATION |
|
|
TRIGGER POINT
Craniosacral Extension: 1. Extension of the ____ bones 2. Sacral base _____ (_____) 3. ___ AP diameter of the cranium 4. _____ rotation of the paired bones Also, is the movement of the sacrum equivalent to inhalation or exhalation? |
Craniosacral Extension:
1. Extension of the _Midline_ bones 2. Sacral base _Anterior_ (_nutation_)[remember nod forward] 3. _Increased_ AP diameter of the cranium 4. _Internal_ rotation of the paired bones Also, is the movement of the sacrum equivalent to inhalation or exhalation? EXHALATION REMEMBER: EXHALATION=CRANIOSACRAL EXTENSION (with respect to direction of the pelvis) |
|
|
Describe a cranial torsion
|
sphenoid rotates one way, the occiput rotates the opposite
named for the greater wing of sphenoid that is more superior |
|
|
sphenoid is rotate so that the greater wing of the sphenoid is more inferior on the right...
what is this? |
Left cranial torsion
remember you name for the greater wing that is more SUPERIOR |
|
|
what are the pathologic and physiologic strain patterns in cranial?
|
pathologic:
Flexion/extension Vertical strain Lateral strain Compression Physiologic: Right/left Torsion Sidebending/Rotation (L or R) |
|
|
if the SBS deviates caudad what type of strain do you have?
|
Extension
|
|
|
if the SBS is deviated cephalad
|
flexion
|
|
|
how can you tell the difference btw a superior and inferior vertical strain?
|
Superior: sphenoid base deviates cephalad in relation to the occiput (greater wings point down)
Inferior: sphonoid base deviates caudad in relation to the occiput |
|
|
if the greater wing of sphenoid deviates left what is the strain pattern?
right? |
Left: left lateral strain
right: right lateral strain |
|
|
TRIGGER POINT
this type of strain occurs when the sphenoid and occiput have been pushed together..... what will your CRI be like? Cause? |
Compression
Decrease in the amplitude of flexion and extension components of the CRI due to trauma to the back of the head |
|
|
Where do V1 V2 and V3 exit the cranium respectively?
|
V1: Superior orbital fissure
V2: Foramen Rotundum V3: Ovale |
|
|
Where does CN VII exit the cranium?
|
enters internal acoustic meatus and exits the stylomastoid foramen
|
|
|
TRIGGER POINT:
What 3 nerves can lead to suckling dysfunction in the newborn? What is the tx? |
CN IX
CN X CN XII Occipital/condylar decompression |
|
|
TRIGGER POINT:
Vagal somatic dysfunction can be due to dysfunction at what 3 places? |
OA
AA C2 |
|
|
TRIGGER POINT:
Dysfunction of CN __ can cause tinnitus, vertigo, or hearing loss |
CN VIII
|
|
|
What is venous sinus drainage
|
Operator spreads apart the sutures of the cranium that overly the occipital, transverse, and sagittal sinuses
|
|
|
This tx can be used to enhance the amplitude of the CRI by resisting the flexion phase and encouraging the extension phase of the CRI until a still point is reached, then allowing restoration of normal flexion and extension. It has been reported to be helpful in fluid homeostasis and help induce uterine contractions
|
CV4: Bulb decompression
|
|
|
TRIGGER POINT:
What tx will increase the amplitude of the CRI? (and fluid homeostasis and uterine contractions) |
CV4
|
|
|
Where do you put your fingers in the vault hold?
|
Index: greater wing of sphenoid
Middle: Temporal bone in front of the ear Ring Finger: Mastoid region of the temporal bone Little finger: squamous portion of the occiput |
|
|
what technique is used to separate restricted or impacted sutures?
which is used to aid in the balance of membranous tension? |
Vspread
Lift (frontal or parietal) |
|
|
Dentistry, newborn babies, or car accidents can all be times to do what?
|
cranialsacral tx
|
|
|
absolute contraindications of cranial? 3
|
acute intracranial bleed or increased intracranial pressure (CNS malignancy or infection)
Skull fracture Relative: seizure history or traumatic brain injury |
|
|
What are the unpaired bones? 5
how do they move? |
Unpaired bones move in flexion/extension
Ethmoid Mandible Occiput Sphenoid Vomer |
|
|
In a sidebending rotation how do the sphenoid and occiput move in relation to each other?
|
they rotate the same way!!
remember: in torsion they rotate opposite ways...this can help you pick btw these 2 |
|
|
What is Facilitation?
|
the maintenance of a pool of neurons (like those in a ganglion) in a state of partial or sub threshold excitation
this makes it so less afferent stimulation is needed to trigger the discharge of impulses A facilitated segment can lead to TART (tissue texture change, asymmetry, restriction, tenderness) |
|
|
what is the difference btw a viscero-somatic reflex and a somato-visceral reflex
|
viscero-somatic: cholecystitis refers pain to the thoracic region at the tip of the right scapula
somato-visceral: trigger point in the right pectoralis major can cause arrhythmia |
|
|
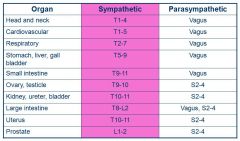
Make sure you are aware of the parasympathetic and sympathetic functions of organs
|
this is a table on p.102, it is pretty straight forward but if you are shaky go look at it
|
|
|
What 2 parasympathetic ganglion does CNVII travel to, and what are their functions
|
Sphenopalatine: lacrima and nasal glands
Submandibular: Submandibularand sublingual glands |
|
|
What is the name of the PARAsympathetic nerve that comes off at S2/3/4
|
Pelvic splanchnic
note: Lumbar/Sacral are SYMPATHETIC |
|
|
Please give the sympathetic and parasympathetic spinal reflex levels for:
Head and neck |
Symp: T1-4
Para: Vagus |
|
|
Please give the sympathetic and parasympathetic spinal reflex levels for:
Cardiovascular |
Symp: T1-5
Para: Vagus |
|
|
Please give the sympathetic and parasympathetic spinal reflex levels for:
Respiratory |
Symp: T2-T7
Para: Vagus |
|
|
Please give the sympathetic and parasympathetic spinal reflex levels for:
Stomach |
Symp: T5-T9
Para: Vagus |
|
|
Please give the sympathetic and parasympathetic spinal reflex levels for:
Liver |
Symp: T5-T9
Para: Vagus |
|
|
Please give the sympathetic and parasympathetic spinal reflex levels for:
Gall bladder |
Symp: T5-T9
Para: Vagus |
|
|
Please give the sympathetic and parasympathetic spinal reflex levels for:
Small intestine |
Symp: T9-11
Para: Vagus |
|
|
Please give the sympathetic and parasympathetic spinal reflex levels for:
Ovary |
Symp: T9-10
Para: S2-4 |
|
|
Please give the sympathetic and parasympathetic spinal reflex levels for:
Testicle |
Symp: T9-10
Para: S2-4 |
|
|
Please give the sympathetic and parasympathetic spinal reflex levels for:
Kidney |
Symp: T10-11
Para: S2-4 |
|
|
Please give the sympathetic and parasympathetic spinal reflex levels for:
Ureter |
Symp: T10-11
Para: S2-4 |
|
|
Please give the sympathetic and parasympathetic spinal reflex levels for:
Bladder |
Symp: T10-11
Para: S2-4 |
|
|
Please give the sympathetic and parasympathetic spinal reflex levels for:
Large intestine |
Symp: T8-L2
Para: Vagus and S2-4 |
|
|
Please give the sympathetic and parasympathetic spinal reflex levels for:
Uterus |
Symp: T10-11
Para: S2-4 |
|
|
Please give the sympathetic and parasympathetic spinal reflex levels for:
Prostate |
Symp: L1-2
Para: S2-4 |
|
|
What sympathetic level is the Adrenal Medulla at?
Appendix? |
Medulla: T10
Appendix: T12 |
|
|
What is the parasympathetic innervation of the GI system
|
entire small intestine: vagus
Proximal large intestine (ascending and transverse)= Vagus Distal half= descending and recto-sigmoid= Pelvic Splanchnic |
|
|
What are the sympathetic innervations of the upper extremities?
|
T2-T8
|
|
|
in the GI, what is the sympathetic innervation after the splenic flexure?
|
T12-L2
|
|
|
What is the purpose of Rib raising?
|
Normalize (decrease) sympathetic activity and improve lymphatic return as well as encourage maximum inhalation
will help thin mucous secretions reduce post surgical ileus |
|
|
What is the purpose of soft tissue paraspinal inhibition ? use?
|
normalize (decrease) sympathetic activty
ileus prevention (has same effect as rib raising) |
|
|
purpose of celiac ganglion, superior mesenteric, inferior mesenteric release?
|
normalize (decrease) sympathetic activity
|
|
|
how do you tx Chapman's points? Purpose?
|
Soft circular manipulation over the point itself
decrease sympathetic tone to associated visceral tissues |
|
|
Person has thick nasal secretions...what is a potential treatment targeted at parasympathetics?
|
Sphenopalatine ganglion technique
manual finger pressure intraorally leads to thin watery secretions |
|
|
TRIGGER POINT:
A newborn is having difficulties suckling, what treatment could you do to help this? what was the cause |
the kid may have condylar compression
tx with Condylar decompression! |
|
|
If you want to treat parasympathetics for autonomic issues, where are you going to target your tx?
|
at the OA, AA, C2
|
|
|
Sympathetic innervation to gonads?
|
T9-10
|
|
|
Draw out the Foundations autonomic chart
|
|
|
|
smooth, firm, discretely palpable nodules, approximately 2-3mm in diameter, located within the deep fascia or on the periosteum of a bone. This describes?
|
a Chapman's Point
|
|
|
Gentle pressure here will elicit a sharp nonradiating and exquisitely distressing pain
|
a chapman point
|
|
|
do chapman's points show somato-visceral or viscero-somatic reflexes?
|
Viscero-somatic
they are a somatic manifestation of a VISCERAL DYSFUNCTION |
|
|
Where is the chapman point for the Appendix?
|
Anteriorly: tip of the right 12th rib
Posterior: transverse process of T11 |
|
|
Where is the chapman point for the Adrenals?
|
ant: 2" superior and 1" lateral to the umbilicus
posterior: between the spinous and transverse processes of T11 and L1 |
|
|
Where is the chapman's point for the kidneys?
|
Ant: 1" superior and 1" lateral to umbilicus
Post: btw the spinous and transverse processes of T12 and L1 |
|
|
Where is the Chapman's reflex point for the bladder?
|
Periumbilical region
|
|
|
Where are the chapman's points for the colon?
|
lateral thigh, within the IT band from greater trochanter to just above the knee
|
|
|
Where is the Chapman point for the middle Ear?
|
ant: superior to medial clavical
post: C1 post rami |
|
|
Where is the Chapman point for the sinuses
|
ant: inferior to medial clavicles
post: C2 articular pilars |
|
|
Where is the Chapman point for the ovaries?
|
ant: pubic tubercles
post: T10 transverse process |
|
|
Where is the Chapman point for the urethra?
|
ant: pubic tubercles
post: L3 transverse process |
|
|
Where are the Chapman's points for the prostate?
|
ant: lateral IT bands
post: PSIS |
|
|
Where is the Chapman's point for the Gall Bladder?
|
ant: Right medial 6th intercostal space
post: Right T6 transverse process |
|
|
This is a hypersensitive focus usually within a taut band of skeletal muscle or in the muscle facia. It is painful upon compression and can give rise to a characteristic referred pain tenderness and autonomic phenomena
|
Trigger Point
|
|
|
Tx for trigger points?
|
Spray and stretch
Injection with local anesthetic ME MFR |
|
|
TRIGGER POINT:
Which may refer pain when pressed, a trigger point or a tenderpoint? |
Trigger points may refer pain when pressed
Tenderpoints DO NOT refer pain when pressed |
|
|
direct and indirect MFR are done via moving towards a barrier or away. But additionally, compression or traction can be done. Which of the above applies to direct and indirect respectively?
|
Traction: Direct
Compression: indirect |
|
|
TRIGGER POINT:
list the 5 steps of MFR |
1. palpate restriction
2. Apply compression (indirect) or traction (direct) 3. Add twisting or transverse forces 4. Use enhancers 5. Await release |
|
|
restoring functional baland and improving lymphatic flow are the goals of what tx?
|
MFR
|
|
|
Where are the 4 compensatory curve locations?
|
OA
Cervicothoracic junction thoracolumbar junction Lumbosacral junction 80% have OA rotated left, CT right, TL left, and LS right |
|
|
what is the Common compensatory pattern of fascia?
|
80% have OA rotated left,
CT right, TL left, and LS right |
|
|
When performing indirect MFR what barrier is engaged?
|
anatomic
|
|
|
What lymphatic tx is particularly useful for pediatric pts?
|
pedal pump
improves total body lymphatic movement |
|
|
when treating a pt for lymphatic problems, what do you tx first?
|
Thoracic inlet
unless contraindicated (rib fracture) |
|
|
what is the goal of rib raising?
|
to normalize hypersympahtetic activity
|
|
|
osseous fractures
bacterial infections with temp greater than 102 abcess carcinoma are all realtive contraindications to what type of tx? |
Lymphatic
|
|
|
the right extremity and right hemicranium and what 2 other organs drain to the right minor lymphatic duct? (everything else drains to the left)
|
heart and lungs (minus upper left lobe)
|
|
|
restriction in sibson's fascia can produce edema where?
|
entire body
this is the thoracic inlet |
|
|
what is attributed to Alpha-Gamma regulation:
trigger point or tenderpiont? |
tenderpoint
found at origin, insertion, or belly of striated muscle |
|
|
where are most maverick points located? how do you tx them
|
Cervical region
position opposite of what is used typically |
|
|
why do you hold a counterstrain point for 90 seconds?
|
this is the time required for the proprioceptive firing to decrease in frequency and amplitutde
|
|
|
for an anterior cervical tenderpoint how do you position the pts head?
|
side bend and rotate AWAY from the side of the tp
|
|
|
for cervical and thoracic tenderpoints how do you sidebend and roate?
Do you flex or extend when treating an anterior tp? posterior? |
Rotate and sidebend away
for anterior flex posterior extend |
|
|
on the ribs, anterior tenderpoints are associated with depressed or elevated ribs? posterior?
how long do you hold? |
anterior: depressed ribs
posterior: elevated ribs 120s |
|
|
TRIGGER POINT:
where is the anterior tenderpoint for L5 located? |
one cm lateral to the pubic symphysus on the superior ramus
|
|
|
where is the iliacus TP?
|
7cm medial to the ASIS
|
|
|
what type of contraction is done in ME? when this occurs, what senses the change in tension and gives a reflex relaxation?
|
Isometric contraction (distance btw origin and insertion stays the same)
Golgi tendon organs |
|
|
Post surgical pts and intensive care pts should not undergo this active technique
|
ME
|
|
|
how do you diagnose the OA
|
triplanar
rotation and sidebending occur in different directions |
|
|
What is the key rib in an inhalation dysfunction?
if you are treating ribs 1-5, what kind of rib is this? do you flex or sidebend? |
Lowest in the group
1-5: pump handle--flex 6-10: bucket handle--sidebend |
|
|
given the following ribs, match the muscle that corresponds with their inhalation dysfunction:
Rib 1 Rib 2 Ribs 3-5 Ribs 6-9 Ribs 10-11 Rib 12 Match With: Quadratus lumborum Posterior scalene Serratus anterior Latissimus Dorsi pectoralis minor Anterior and middle scalene |
Rib 1: Anterior & Middle scalene
Rib 2: Posterior Scalene Ribs 3-5: Pectoralis Minor Ribs 6-9: Serratus anterios Ribs 10-11: Latissimus Dorsi Rib 12: Qudratus Lumborum |
|
|
Osteoprosis
Osteomyelitis Fractures Bone metastisis are all what for what tx? what are 2 more (one is a autoimmune dz, another is a genetic problem)? reason? |
ABSOLUTE contraindications of HVLA
Rheumatoid arthritis (transverse ligament of the dens is weak and cervical manipulation can lead to AO sublux and neuro damage) Downs Syndrome (same as above) |
|
|
Acute whiplash
Pregnancy Post-surgical Herniated nucleus propulsus anticoagulant therapy vertebral artery ischemia Are all what for what tx? |
Relative contraindications
HVLA |
|
|
When treating a flexed lesion with the Kirksville Krunch, what segment do you treat? What direction is the thrust aimed at?
What about for an extended segment |
Flexed: treat the dysfunctional vertebrae; thrust aimed at floor
Extended: vertebrae below, thrust aimed 45 degrees cephalad |
|
|
articulatory techniuqes use what kind of motion
|
springing
good for elderly and post op pts rib raising is an example of articulatory |
|
|
this technique is good for pts with inactivity or adhesive capsulitis following an injury
|
Spencer Technique
|
|
|
What is the spurling test?
|
extend and sidebend C-spine to side being tested and push down
test is positive if pain radiates into ipsilateral arm normally due to narrowing of the neural foramina |
|
|
What is the Wallenberg test?
|
test vertebral artery insufficiency
rotate/side bend neck to each side positive test results when pt is dizzy or visual change, etc shows problem on other side |
|
|
What is Adson's Test
|
test for thoracic outlet syndrome
arm extended at elbow, shoulder is extended, externally rotated and slightly abducted. Pt bends head toward ipsilateral arm test is positive with a severely decreased or absent radial pulse due to tight scalene muscles |
|
|
What is the Wright Test?
|
neurovascular bundle test
as it passes under the pectoralis minor muscle at the coracoid process hyperabduct the arm above the head with extension |
|
|
What is the costoclavicular syndrome test? (military posture test)
|
checks compression of the neurovascular bundle btw the clavicle and 1st rib
palapate radial pulse while depressing and extending the shoulder |
|
|
What does the Apley scratch test show
|
ROM of the shoulder
|
|
|
Drop arm test shows what
|
tear of the rotator cuff
have pt slowly lower the arm positive test if the pt cannot lower smoothly |
|
|
What is the Speed's Test?
|
tests biceps tendon in bicipital groove for pain
have pt flex against resistance |
|
|
What is the Yergason's Test?
|
determines the STABILITY (vs pain in the Speed's test) of the biceps tendon in the bicipital groove
have pt flex while you pull down on the elbow and externally rotate pain due to biceps tendon popping out of the groove |
|
|
What is the Allen's test?
|
tests blood supply to hand
occulde ulnar and radial arteries at wrist let go of one and see if blood goes into hand. repeat w/ other artery |
|
|
What is the Finkelstein test?
|
test for tenosynovitis in the abductor pollicis longus and extensor pollicis brevis tendons at the wrist (De Quervain's dz)
tuck thumb into fist, ulnar deviate, look for pain |
|
|
Phalens test?
|
test for carpal tunnel
flex wrists, look for tingling |
|
|
Tinnel test
|
tap over the volar aspect of the pts transverse carpal ligament
postive test cuases tingling or paresthesia into thumb index, middle and lat half of ring finger |
|
|
TRIGGERPOINT:
What is the purpose of the hip drop test? How is it done? What is the important degree change you must see for a positive test? |
elvauates side bending of the lumbar spine
have pt bend one knee without lifting the heel from the floor. Normall the spine should sidebend toward the side contralateral to the bending knee producing a convexity on the ipsilateral side the ipsilateral crest should drop 20-25 degrees positive test is indicated by anything less than a smooth convexity in the lumbar spine or a drop of the iliac crest less than 20-25 degrees |
|
|
What is the straight leg test? How can you distinguish the 2 things it shows
|
pt lies down. lift leg to 70 degrees
if pain, it is either hamstring tighness or sciatic n. dorsiflex the foot (Braggards test)-->if painful then it is sciatic |
|
|
What do the Seated flexion test and standing flexion test show respectively?
COMBANK has a hard on for this |
seated: sacroiliac
standing: iliosacral |
|
|
What is the pelvic side shift test? what is it often seen in?
|
determines if the sacrum is midline
test is positive on the side of freer translation, this indicates the pelivis is shifted to that side often seen in a flexion contracture of the iliopsoas (psoas syndrome) |
|
|
What is the Trendelenberg test?
|
assesses the gluteus medius muscle strength
pt picks one leg off the floor. normally you should have a even pelvis supported by the glut med. positive test occurs when the pelvis falls, which indicates weakness in the glueus medius muscle positive right trendelenberg indicates left gluteus medius weakness |
|
|
TRIGGER POINT:
The lumbosacral spring test will be (positive/negative) in all the dysfunctions in which the sacral base moves posterior |
POSITIVE
|
|
|
What is the Ober's test?
|
detects tight tensor fascia lata and IT band
pt lies on side opposite that being tested. Flex knee to 90, abduct the hip as far as possible. Slightly extend the hip while stabilizing the pelivs to keep from rolling Test is positive if the thigh remains abducted as the physician allows the leg to fall to the table |
|
|
What is the Patrick's Test (FABERE)
|
tests pathology of SI and hip joint (especially osteoarthritis of the hip)
FABERE=Flexion Abdution External Roation Extension so a figure four position (indian style but with 1 leg) any pain shows pathology of that hip joint |
|
|
What is the Thomas test?
|
tests a flexion contracture of the hip (iliopsoas)
pt lies down on back, flex hip so knee hits abdomen if other leg lifts off table-->positive test and contracutre of the iliopsoas |
|
|
difference btw anterior draw test and Lachmans?
|
ant: 45 degrees flexion
lach: 30 degrees and more accurate both test ACL |
|
|
What is the Bounce Home test?
|
evaluates problems with full knee extension looking for meniscal tears or joint effusions
pt supine, grab heel and flex it, drop it and let it go to extension knee should "bounce home" into full extention positive test if it doesn't |
|
|
What is the Apley Compression ad Distraction test?
|
Compression: Maniscus tear
-press down, and internal/external rotate-->pain=positive test Distraction: MCL/LCL test -pull up, internal/external roate the tibia->pain=positive |
|
|
What is McMurray's Test?
|
detects tears in the posterior aspect of menisci
flex knee, external rotate to valgus position, extend knee. If click= positive test=tear of posterior medial meniscus same is done with varus stress for lateral |
|
|
you push the knee medial, what test is this?
|
lateral force is the valgus stress test
if gapping occurs you have MCL tear |
|
|
you push the knee laterally, what are you testing for
|
LCL tear
varus stress testing |
|
|
the trendelenberg test will assess which of the following muscle groups:
hip extensors flexors aBductors aDductors external rotators |
aBductors
remember this tests the gluteus medius muscle |
|
|
describe how you would position a patient for ME to treat an anterior and posterior innominate rotation
supine/prone flex leg or extend etc |
ANTERIOR: with patient supine, flex patient's right knee and hip, ask patient to push against you for 3-5 seconds, re-engage the barrier; repeat 3-5 times
POSTERIOR: with patient supine, extend patient's right leg and innominate off the table, ask patient to push leg anteriorly for 3-5 seconds, re-engage the barrier; repeat 3-5 times |
|
|
Click to toggle an attachment list
A young mother brings in her 2 week old infant concerned that the baby still has not “gotten the hang of feeding” You evaluate the infant and discover that she has a very poor suck reflex. To correct the identified dysfunction you first perform: ( A ) CV4 technique Cross/Uncross out this answer ( B ) Condylar decompression Cross/Uncross out this answer ( C ) Balancing of the temporals Cross/Uncross out this answer ( D ) SBS decompression Cross/Uncross out this answer ( E ) Correction of the sphenoid strain pattern Cross/Uncross out this answer |
( B ) Condylar decompression
When the XIIth cranial nerve is compressed and causing poor sucking in an infant condylar decompression should be performed. Compression of the 4th ventricle (CV4) technique has value to stimulate the newborn, but this infant has a clear cut problem which should be corrected before moving on to other techniques. Balancing of the temporals would help with nerve dysfunction of the cranial nerves that have some association with the temporal bones which are CNIII through XI. This child has no indication of having an SBS compression and therefore the necessity of decompression is unlikely. Correction of the sphenoid strain pattern should help with nerve dysfunction of related nerves which includes: CNI-CNVIII. |