Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
60 Cards in this Set
- Front
- Back
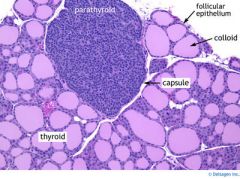
What is this?
|
Normal Thyroid and parathyroid!
|
|
|
Explain NORMAL embryological development of the Thyroid Gland.
Where does it originate? |
The Thyroid gland originates at the base of the tongue and extends down the to the anterior neck. The duct which goes down gets involuted (deleted).
|
|
|
What is Thyroglossal Duct Cyst?
Where does the mass appear? |
The duct is the connection from where the Thyroid began developing (base of tongue) to its final location (anterior neck)
The duct fails to involute (delete) during development. A persistent duct may undergo cystic dilation Anterior Neck mass |
|
|
What is Lingual Thyroid?
|
Persistence of the thyroid at the base of the tongue (doesn't extend down).
Presents as a base of tongue mass |
|
|
Basic principles of Hyperthyroidism? (2 things it increases and MOA)
|
Increased basal metabolic rate (increased Na/K ATPase synthesis)
Increases sympathetic nervous system (Increased in beta receptor) |
|
|
Common symptoms of hyperthyroidism?
|
Weight loss, despite increased appetite
Heat intolerance, sweating tachycardia arrhythmia Diarrhea Bone resoprtion (osteoporosis) Hypocholesterolemia Hyperglycemia (gluconeogensis and glycongenolysis) |
|
|
What is Grave's Disease?
|
IgG autoantibody that stimulates TSH receptor (type II hypersensitivity)
Increased synthesis and release of thyroid hormone Most common cause of hyperthyroidism Women of childbearing age: most common group |
|
|
What is the most common cause of hyperthyroidism?
|
Grave's Disease
|
|
|
What type of hypersensitivity reaction is Grave's disease?
What type of autoantibody? |
Type II
IgG |
|
|
Clinical features of Grave's disease
|
Hyperthyroidism
Diffuse goiter Exophthalmos (bulging of the eye anteriorly) Pretibial myxedema-nonpitting scaly thickening and induration of the skin |
|
|
Common symptoms of Grave's disease?
|
Weight loss, despite increased appetite
Heat intolerance and sweating Tachycardia Arrhthmia Diarrhea Hypocholesterolemia Hyperglycemia |
|
|
What is diffuse goiter?
|
Diffuse goiter is the enlargement of the thyroid in a diffuse manner.
(due to hyperplasia and hyperthrophyy of thyroid due to overstimulation by "TSH") |
|
|
MOA behind Exophthalmos and pretibial myxedema
|
Fibroblasts behind the orbit and shin express TSH receptor
TSH activation results in glycosaminoglycan buildup leading to inflammation, fibrosis and edema |
|
|
What molecule/material builds up in Exophthalmos and pretibial myxedema?
What is it stimulated by? |
Glycosaminoglycan
Stimulated by TSH |
|
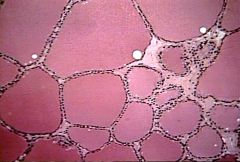
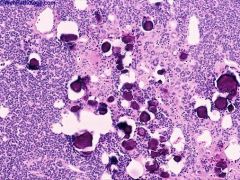
What is this?
|
Diffuse Goiter
(Would also see chronic inflammation) |
|
|
Lab findings of Grave's disease? (4)
|
Increased total and free T4.
Decreased TSH Hypocholesterolemia Hyperglycemia |
|
|
What is the most fatal complication of Grave's disease?
|
Thyroid storm!
|
|
|
What is thyroid storm?
When does it occur? Symptoms? |
Fatal complication of Grave's disease.
Too much catecholamines (sympathetic) in response to stress (injury, surgery, birth, etc.) Presents as arrhthymia, hyperthermia, vomiting, hypovolumic shock |
|
|
What is Multinodular goiter?
Etiology? Consequences? |

Enlargement of thyroid with multiple nodules
Due to decrease iodine Usually nontoxic (euthyroid - "normal" thyroid) Rarely, toxic goiter |
|
|
What is toxic goiter?
|
Rare consequence of multinodular goiter.
Regions become TSH independent leading to hyperthyroidism (release on their own) |
|
|
Common symptoms of hypothyroidism?
|
All due to decreased metabolic rate and decreased sympathetic nervous system.
Weight gain, despite normal appetite Cold intolerance Constipation Bradycaria Hypercholesterolemia Myxedema (due to glycosaminoglycans in skin) |
|
|
Cretinism vs. Myxedema
(age group?) |
Cretinism - hypothyroidism in neonates + infants
Myxedema - hypothyroidism in older children + adults |
|
|
Cretinism
Common symptoms |
Hypothyroidism in neonates + infants
Mental retardation, short stature with skeletal muscle abnormality, weird facial features, enlarged tongue, and umbilical hernia Thyroid needed for brain + skeletal development |
|
|
Etiology of Cretinism
|
Maternal hypothyroidism during pregnancy
Thyroid agenesis Iodine deficiency Dyshormonogenetic goiter - congenital defect in thyroid hormone production |
|
|
Myxedema
Common symptoms? |
Hypothyroidism in older children and adults
All due to decreased metabolic rate and decreased sympathetic nervous system. Weight gain, despite normal appetite Cold intolerance Constipation Bradycaria Hypercholesterolemia Myxedema (due to glycosaminoglycans in skin) |
|
|
Etiology of Myxedema
|
Most common causes: iodine deficiency and Hashimoto thyroiditis
Other causes: drugs (lithium), surgical removal, radioablation of thyroid |
|
|
What are the most common causes of Myxedema?
|
Iodine deficiency and Hashimoto Thyroiditis
|
|
|
What is Hashimoto thyroiditis?
Associated with what HLA? Most common cause of hypothyroidism in regions where ___________ are adequate |
Autoimmune destruction of the thyroid glands
Associated with HLA-DR5 Most common cause of hypothyroidism in regions iodine levels are adequate |
|
|
Clinical features of Hashimoto thyroiditis
|
Hyperthyroidism initially b/c all the stored thyroid all thrown out due to follicle damage
Progresses to hypothyroidsm (low T4, high TSH) Antithyroglobulin and antimicrosomal antibodies (they aren't the cause; MARKERS) |
|
|
name 2 antibody markers for Hashimoto thyroiditis
|
Antithyroglobulin and antimicrosomal antibodies
|
|
|
Is there an initial increase or decrease in thyroid in Hashimoto thyroiditis? Why?
|
Increase b/c the damage follicle cells release all the stored thyroid
|
|
|
Common histological finding of Hashimoto thyroiditis?
|
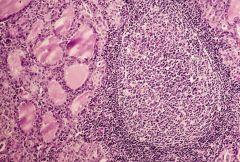
Chronic inflammation with germinal centers and Hurthle cells (eosophillic aka PINK)
|
|
|
What are Hurthle cells?
Associated with what disease? |
Eosinophilic metaplasia of cells that line follicles
Associated with Hashimoto thyroiditis (normally NOT pink) |
|
|
What are you at an increased risk of if you have Hashimoto Thyroiditis (what cancer?)
|
B-cell (marginal zone) lympoma
presents as an enlarged thyroid gland then |
|
|
Subacute Granulomatous (De Quervain) Thyroiditis
Prognosis? |
Granulomatous thyroiditis that follows a viral infection
Presents as a TENDER* thyroid with transient hyperthyroidism Self-limited (doesn't progress to hypothyeroidsm) |
|
|
What is tender thyroid associated with?
|
Subacute thyroiditis
|
|
|
Reidel Fibrosing Thyroiditis
|
Chronic inflammation with extensive fibrosis of the thyroid gland
"hard as wood" nontender thyroid gland with hypothyroidism Fibrosis may extend to involve local structures (airway, esophagus); mimics anaplastic carcinoma but these pt. are YOUNGER |
|
|
What does Reidel Fibrosing Thyroiditis mimic?
How do you differentiate? |
Mimics anaplasic carcinoma
But RFT pt. are younger and on biopsy don't have malignant cells |
|
|
What is "hard as wood non tender thyroid gland" associated with?
|
Reidel fibrosing thyroiditis?
|
|
|
Why might you get Dysphagia and trouble breathing with Reidel fibrosing Thyroiditis?
|
The fibrosing may spread from the thyroid to nearby structures
|
|
|
Thyroid Cancers
Basic principles - multiple or solitary nodules? -Most benign or malingant? |
Usually presents as a distinct solitary nodule
Most are benign |
|
|
What studies are used to further characterize a nodule?
|
Radioactive Iodine (131) uptake studies
|
|
|
Increased uptake of iodine on radioactive uptake studies suggests what diseases?
|
Suggests grave's disease or nodular goiter
('hot nodules b/c hyperthyroidism) |
|
|
Decreased uptake of Iodine on radioactive uptake studies suggest what diseases?
What is the next step? |
CANCERs
Adenoma and carcinoma BIOPSY! |
|
|
When should you biopsy? (increased or decreased uptake of Iodine in radioactive uptake studies?)
What kind of bioposy? |
Decreased uptake MAY indicate cancer thus biopsy!
Fine needle aspiration biopsy! |
|
|
Follicular adenoma
Functional or non-functional? Benign or malignant? |
Benign proliferation of follicles surrounded by capsule
Usually nonfunctional (doesn't secrete thyroid) |
|
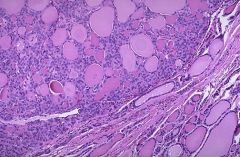
What is this? How can you tell?
|
Follicular adenoma
(looking at the picture, you can tell the top looks different from bottom. The seperation is the CAPSULE.) Benign |
|
|
4 types of carcinomas of the Thyroid
|
Papillary, Follicular, Medullary, Anaplastic
|
|
|
How do MOST carcinomas spread?
(via blood or lymph node) 4 common exceptions? |
MOST spread via lymph nodes
Renal cell carcinoma, hepatocellular carcinoma, choriocarcinoma, follicular carcinoma are the exception! |
|
|
What is the most common type of thyroid carcinoma?
|
Papillary carcinoma
|
|
|
Papillary carcinoma
Risk factor/Etiology? Appearance (histology) Spread where? Prognosis? |
Most common type of thyroid carcinoma
Risk factor: exposure to ionizing radiation in childhood Histology: 'Orphan Anni eye nuclei' nuclear grooves associated with psammoma bodies Spread to cervical lymph nodes GREAT prognosis |
|
What is this (the white clearing in the nucelus)?
Associated with what disease? |
Orphan Annie eye nuclei (clear white in nucleus)
Seen in Papillary carcinoma (all types including Thyroid) |
|
|
What are Psammoma bodies?
|
Round collection of calcium seen microscopically
(picture shows Papillary carcinoma of the kidney. But just shows you psamma bodies!) |
|
|
Follicular Carcinoma
Benign or Malignant? It is an exception to what rule? |
Malignant proliferation of follicles surrounded by capsule but this INVADES past the capsule
Exception to the rule that carcinomas spread via lymph nodes. This spreads via BLOOD. |
|
|
What is the difference b/w follicular carcinoma and adenoma?
Can Fine needle aspiration help distinguish? |
Adenoma doesn't invade pass the capsule
FNA only examines cells and not the capsule thus it doesn't help you distinguish the difference |
|
|
Medullary carcinoma
Benign or malignant? Histology? Genetics? |
Malignant proliferation of C cells
Histology: sheets of malignant cells in an amyloid stroma If it is genetic then it is related to multiple endocrine neoplasia (MEN 2A and 2B) These are associated with mutations in RET oncogene |
|
|
What to do with thyroid if RET mutation found?
|
Prophylacit thyroidectomy
|
|
|
What is the role of C cells? What is the role of its product released?
What does calcitonin deposit within the tumor as? What cancer causes proliferation of C cells? |
C cells produce calcitonin
Calcitonin decreased calcium Calcitonin depositins within the tumor as amyloid Medullary Carcinoma |
|
|
Calcitonin
|
Decreases calcium
Hypocalciemia |
|
|
Anaplastic Carcinoma
What age group? What can it be confused with? How do you differentiate? Prognosis? |
Undifferentiated malignant tumor of the thyroid
Seen in elderly Can be confused with Reidel Fibrosing Thyroditis (age + biopsy differ b/w the two) Invades local structures such as esophagus and throat Poor prognosis |