Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
60 Cards in this Set
- Front
- Back
|
18 year-old male
Fever, confusion, nausea 4 days after general anesthesia Elevated AST, ALT, bilirubin Diagnosis Pathophys Histologic Findings |
Halothane-associated hepatitis
Halogenated inhalation anesthetics (halothan, enflurane, isoflurane, sevoflurane) can cause cause severe liver damage. Esp. halothane bc it's most extensively metabolized in liver. Light microscopy will reveal widespread hepatic necrosis due to direct liver injury by halothane metabolites and formation of autoab's x liver proteins. |
|
|
How do gram-positive bacteria differ from gram-negative bacteria (structurally/functionally)?
|
Gram positive organisms have a cytoplasmic membrane composed of phospholipid bilayer IN ADDITION to a peptidoglycan cell wall outside of that cell membrane.
The peptidoglycan cell wall provides shape of bacterium as well as resistance to osmotic stress. |
|
|
Which antibiotics inhibit the 30S bacterial ribosome subunit?
50S? |
30S: Tetracyclines, Aminoglycosides
50S: Chloramphenicol, Macrolides |
|
|
Which antibiotics disrupt the peptidoglycan cell wall of Gram-positive and Gram-negative organisms?
|
PCN
Cephalosporins Vancomycin |
|
|
What is the most common cause of fetal hydronephrosis (embryological processes, specific region of hydronephrosis)?
|
During development, the ureters are fully canalized before the metanephros (which branches to form the collecting ducts, calices, renal pelvis, ureters, and renal parenchyma) begins to produce urine.
Occasionally, the metanephros will begin producing urine before canalization of the ureteric bud is complete and this leads to a transient hydronephrosis. Occurs at the ureteropelvic junction (junction between kidney and ureter--last of the ureter to canalize). |
|
55 year-old woman
s/p cholecystectomy Sudden onset nausea, fever Viral serologies negative Liver on autopsy DIagnosis Pathophys Lab values |
Inhaled anesthetics, such as halothane, can be associated with lethal fulminant hepatitis that cannot be histologically distinguished from acute viral hepatitis.
Labs will show elevated ALT, prolonged PT time, and elevated eosinophils. |
|
|
How does the presentation of acute liver disease differ from chronic liver disease?
|
Acute: Prolonged PT time, elevated ALT
Chronic: Dec'd albumin (albumin has a half life of 20 days so acute liver failure won't affect it), palmar erythema, ascites, splenomegaly |
|
|
A new drug for treating stable angina has been developed. It inhibits a step in fatty acid oxidation.
What is the most likely MOA explaining its potential benefit? |
Energy for mitochondrial cells mostly comes from fatty acid oxidation in mitochondria (other source =glycolysis, glucose oxidation).
However, fatty acid oxidation requires more oxygen use in comparison to glucose utilization and glycolysis. It's believed that in stable angina, atherosclerosis leads to reduced O2 delivery to cardiac mitochondria, leading to mismatch between mitochondrial O2 demand and supply. Since glucose oxidation requires less O2, it's believed that inhibiting mitochondrial FA oxidation will shift energy production to glucose oxidation (which would be more O2 efficient). |
|
|
What risk does a retained dead fetus pose to a pregnant mother?
|
DIC and progressive hypofibrinogenemia
|
|
|
What are the laboratory findings of DIC?
|
Prolonged PTT, PT
Low PLT and microangiopathic hemolytic anemia Low fibrinogen Elevated fibrin split products (D-dimer) Low Factor V and VIII levels |
|
|
Drugs of choice for absence seizures
MOA? |
Ethosuximide--blocks T-type Ca2+ channels in thalamus
Valproate--blocks T-Type Ca2+ channels AND Na+ channels |
|
|
Drugs of choice for absence seizures in addition to tonic-clonic seizures
MOA? |
Valproate--blocks T-type Ca2+ channels and Na+ channels
|
|
|
Phenytoin:
MOA Specific Use |
Inhibits high frequency firing of Na+ channels
Use in TONIC-CLONIC and STATUS EPILEPTICUS |
|
|
ACE inhibitors:
Potential metabolic disturbances |
ACE inhibitors decrease aldosterone secretion and as a result increase Na+ excretion and potassium retention (HYPERKALEMIA)--not common unless in renal failure or taking K+ sparing diuretic
|
|
|
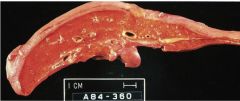
56 year-old male
Long history of dyspnea, wheezing, cough Smoked 2 ppd x 25 years Has been treated with antibiotics when dyspnea is severe Diagnosis |
Chronic bronchitis caused by smoking and exacerbated periodically by superimposed bacterial bronchitis
|
|
|
What is the Reid index?
What does it indicate? |
Reid Index = ratio of thickness of mucus gland layer in bronchial wall submucosa to thickness of bronchial wall between cartilage and respiratory epithelium
It essentially measures mucus gland enlargement Since progressive mucus gland enlargement is the major contributor to bronchial wall thickening in chronic bronchitis (and since increasing wall thickness causes worsening airflow obstruction), elevation of the Reid index above 40% correlates with duration and SEVERITY of CHRONIC BRONCHITIS. |
|
|
What are the specific actions of aldosterone?
|
Increases Na and H2O reabsorption in COLLECTING DUCTS by increasing number of Na/K-ATPase proteins and sodium channels in collecting ducts.
Thus sodium and water are rmemoved from tubular fluid both actively and passively. AS a consequence, K+ and H+ are lost into collecting tubules via secretion from intercalated cells. |
|
|
Osteoporosis:
General definition Type of bone involved |
Loss of total bone mass due to trabecular thinning
Note: trabecular = spongy bone |
|
|
10 year-old male
Headaches, nose bleeds Difficulty walking Pulsatile vessels palpable along ribs Diagnosis Pathophys of findings |
Adult type (postductal) congenital aortic coarctation
Headaches and epistaxis due to HTN in aa supplying head and neck Lower extremity muscle weakness/fatigue due to inadequate lower body perfusion Paplpable intercostal vessels indicate development of collateral arterial circulation to region of aorta distal to coarctation |
|
|
When specifically does an S4 heart sound arise?
Why? |
S4 is heard when there's a sudden rise in end diastolic ventricular pressure caused by atrial contraction against a STIFF LEFT VENTRICLE (ventricle has reached limit of its compliance).
LV stiffness can be due to: Degenerative mitral calcification Aortic valve calcification HTN disease leading to LVH |
|
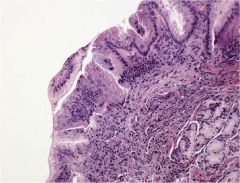
Esophageal biopsy--
Diagnosis |
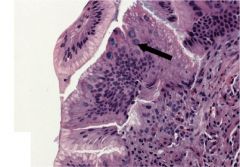
Adenocarcinoma; arrow is pointing to columnar epithelium w/goblet cells (intestinal epithelium). This is diagnostic of Barrett esophagus.
|
|
|
3 year-old male
Recurrent dyspnea relieved by squatting Diagnosis |
TOF
|
|
|
What are the findings of tetralogy of Fallot?
|
PULMONARY STENOSIS (NOT PDA)
RVH Overriding Aorta VSD |
|
|
List the characteristics of drugs that affect the volume of distribution.
Provide the correlating volume of distribution. |
Average total body water is 41 L
ECF volume is 1/3 = 14 L Plasma volume (within ECF) = 3L If drug has large molecular weight, is bound by plasma proteins, or is highly charged (hydrophilic), remains in plasma compartment and Vd: 3-5L If drug has small moelcular weight but is charged (hydrophilic), can distribute ti interstitial fluid as well as intravasc compartment; Vd = 14-16 L If drug has small MW and is uncherged (hydrophobic/lipophilic), can cross cell membranes and reach intracellular compartment; Vd = 41L |
|
|
Significance of low/high AFP during pregnancy.
|
Low AFP: Trisomy 21
High AFP: multiple gestation, NT defects (including spina bifida, anencephaly), omphaloceles and other abdominal wall defects |
|
|
49 year-old female
Ovarian mass with yellow coloration Diagnosed as granulose-theca cell tumor What is it likely to secrete? Effects? |
Likely to secrete estrogen and not androgens.
This will cause precocious puberty in prepubertal girls or fibrocystic change of breast, endometrial hyperplasia/carcinoma in older women. |
|
|
Describe the general path copper takes once ingested.
|
Copper is absorbed in stomach/duode, transported to LIVER via albumin
Within liver, it forms ceruloplasmin Senescent ceruloplasmin and remainder of ingested, unabsorbed copper are secreted into bile and excreted in stool (primary route for copper elimination) YOU POOP IT OUT VIA YOUR LIVER |
|
|
Which CNS tumors stain positively for synaptophysin?
|
Remember: synaptophysin is a protein found in presynaptic vesicles of neurons, neuroendocrine and neuroectodermal cells.
So CNS tumors of NEURONAL ORIGIN will stain positive for synaptophysin. |
|
|
Which CNS tumors stain positively for glial fibrillary acidic protein?
|
CNS tumors of GLIAL origin: astrocytoma, ependymomas, oligodendrogliomas stain positively for GFAP
|
|
|
35 year-old female
Weakness, fatigue, pallor Low RBCs Retic 0.1% BM biopsy reveals absence of erythroid precursors but preserved myeloid and megakaryocytic elements Diagnosis Pathophys Disease associations |
Pure red cell aplasia is a form of marrow failure characterized by hypoplasia of marrow erythroid elements in setting of normal granulopoiesis and thombopoiesis.
It is associated with THYMOMAS and PARVOVIRUS B19 |
|
|
Describe the embryonic formation of the pancreas (doral vs ventral buds).
How does pancreatic divisum arise? Clinical effects? |
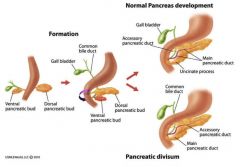
Dorsal bud forms majority of pancreatic tissue (body, tail, most of head)
Ventral pancreatic bud forms the uncinate process, inferior/posterior portion of the head, and major pancreatic duct*** Failure of the dorsal and ventral buds to fuse leads to pancreas divisum where 2 pancreatic ducts open into duodenum (clinically silent; may predispose to dev't of recurrent pancreatitis). |
|
|
What are the symptoms of narcolepsy?
|
Excessive daytime sleepiness with sleep attacks
Hypnagogic (hallucinations while falling asleep) or hypnopompic (hallucinations on waking up) hallucinations Cataplexy (paralysis after laughter/surprise) Sleep paralysis |
|
|
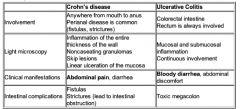
Contrast Crohn's Disease with Ulcerative Colitis in terms of:
Region of bowel involved Light microscopy findings Clinical manifestations Intestinal complications |
|
|
|
32 year-old male
Vague abdominal pain Fever, diarrhea No response to antibiotics Enterocutaneous fistula DIagnosis |
Crohn's (due to transmural inflammn-->fistula)
|
|
|
What side effects of opioid use are most resistant to developing tolerance?
|
Constipation
Miosis (pinpoint pupils) In other words, won't get used to constipation! Need to give laxatives and keep hydrated. |
|
|
Granuloma in lungs:
2 causes |
Tb
Sarcoidosis |
|
|
A study of 400 patients hospitalized with DM-related complications shows that serum cholesterol level is a normally distributed variable with a mean of 220 mg/dL and standard deviation of 10 mg/dL.
Based on the study results how many patients do you expect to have serum cholesterol ≥240 mg/dL in this study? |
240 is 2 SD above mean
So, 95% of patients will be within 2 SD, that is, 95% of patients will be in the range of 200-240 (2SD's in both directions). 5% will be below 200 + above 240. Cut this in half and you have your answer: 2.5% will be above 240. |
|
|
What auscultatory finding would indicate severe mitral regurgitation (beyond holosystolic murmur)?
Why? |
An S3 heart sound
LV S3 gallop indicates increased rate of filling of LV during MID diastole. If there is a high volume of regurgitant flow recycled back into LV during diastole, you will hear an S3. |
|
|
This heart sound is heard when the left ventricle is dilated.
|
S4--predecessor to ventricular failure!!
|
|
|
This heart sound is heard when the left ventricle receives too much fluid during diastole.
|
S3
|
|
|
Calculate the net filtration pressure given:
Glomerular capillary hydrostatic pressure = 45 mmHg Glomerular capillary oncotic pressure = 27 mmHg Bowman capsule hydrostatic pressure = 10 mmHg Bowman capsule oncotic pressure =2 mmHg |
Net filtration pressure = (Pc - Pi) - (πc - πi)
= (45-10) - (27-2) =35-25 =10 mmHg |
|
|
34 year-old man
Fever, chills, dyspnea h/o MVA with emergent laparotomy (2 years ago) BP 80/40 Blood cultures gros S. pneumo Why? |
Patient likely experienced splenic rupture secondary to abdominal trauma 2 years ago, with splenic remnants removed during laparotomy.
Now has impaired bacterial clearance of encapsulated organisms. |
|
|
What is status epilecticus?
|
Recurrent or continuous tonic-clonic seizures that last for more than 30 minutes without a return to consciousness. LIFE-THREATENING.
|
|
|
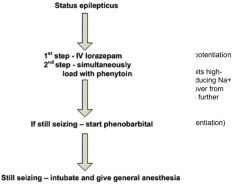
What is the treatment algorithm for status epilecticus?
Include the reason for administering each drug in addition to its MOA. |
|
|
|
Riboflavin:
B vitamin number Signs of deficiency Reaction and enzyme that requires it |
Riboflavin = B2
Deficiency = oral lesions at corners of mouth, anemia, glossitis, eye changes (keratitis, corneal neovascularization) B2 is a precursor of FMN and FAD FAD participates in TCA as a coenzyme of SUCCINATE DH, which converts Succinate into Fumarate |
|
|
VHL Disease:
Presentation Genetic cause (specific mutation) |
Cerebellar hemangioblastomas
Renal clear cell carcinoma Pheochromocytoma VHL Mutation on chromosome 3p |
|
|
Chemotherapeutic that causes:
Finger numbness/tingling How? |
Vinblastine, Vincristine-->interferes w/MT formation in nerve axons
(Affects mitotic spindle; M-phase specific agents) |
|
|
Chemotherapeutic that causes:
Burning on urination and urgency |
Cyclophosphamide or ifosfamide; prevent with mesna
|
|
|
Chemotherapeutic that causes:
Led swelling and orthopnea |
These are signs of heart failure.
Chemo that causes cardiotox = Doxorubucin (intercalating agent) |
|
|
Chemotherapeutic that causes:
Dry cough and exertional dyspnea |
Bleomycin (pulmonary fibrosis)
|
|
|
What regions of the brain are supplied by the ACA, MCA, and PCA?
|

|
|
|
How can fecal-oral viruses be destroyed (in event of contamination)?
|
Water chlorination (bleach 1:100 dilution)
Formalin UV irradiation BOILING for one minute |
|
|
Duodenal ulcer relieved by food
Diagnosis Cause |
Peptic Ulcer Disease caused by H. pylori (or NSAID use)
|
|
|
Thrombophlebitis:
What is it? What does it mean? |
Thrombophlebitis is inflammation of a vein due to a blood clot.
ALWAYS THINK CANCER. It's very common in adenoca of pancreas, colon, lung. Hypercoagulability occurs bc adenoca produce thromboplastin-like substance capable of causing intravasc coagulations that tend to migrate. This is called paraneoplastic syndrome. |
|
|
What is migratory superficial thrombophlebitis?
|
When patient with visceral cancer is in a hypercoagulable state and multiple sites of thrombophlebitis occur. Or one resolves and recurs in another site.
|
|
|
Spoon-shaped nails
|
Iron deficiency anemia
|
|
|
Glomerular basement membrane exhibits irregular spikes
Diagnosis Pathophys |
Membranous glomerulopathy (common cause of nephrotic syndrome in adults)
Can occur secondary to underlying malignant tumors, infections (HBV, HCV, malaria, syphilis), certain meds (gold, penicillamine, NSAIDs). Diffuse inc'd thickness of GBM on light microscopy (without hypercellularity), SPIKE AND DOME APPEARANCE, and granular deposits are diagnostic. |
|
|
56 year-old man
Colon cancer Generalized edema Urine protein excretion 4.5 g over 24 hours Diagnosis Pathophys |
Nephrotic syndrome (losing protein) likely due to membranous glomerulopathy (likely due to underlying malignancy)
|
|
|
Crescendo-decrescendo murmur:
Diagnosis Cause Specific Physical Exam Findings |
Diamond-shaped murmur = AORTIC STENOSIS
MOst common cause = calcification of aortic valve leaflets Physical exam will reveal pulsus parvus et tardus (small and slow rise in carotid pulse during systole) |
|
|
Outline the urea cycle.
Include nitrogen source and the rate limiting step. |
Mitochondria:
CO2 + NH4 + 2ATP + N-ACETYLGLUTAMATE (activates CPS I) --> Carbamoyl phosphate (via CPS I) Carbamoyl phosphate-->Citrulline-->Cytosol Citrulline + Aspartate (NITROGEN SOURCE) -->-->Urea + Ornithine RLS = CPS1 |