Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
12 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
PVT
|
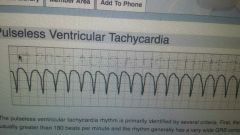
>180bpm, very wide QRS complex
|
originates in VENTRICLE +PULSELESS
|
|
|
Ventricular Fibrillation
|
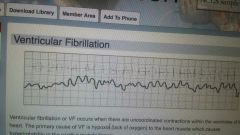
uncoordinated ventricular contractions
|
HYPOXIA primary cause, can lead to ischemia & asystole
|
|
|
Pulseless Electrical Activity PEA
|
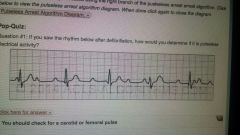
ALWAYS CHECK FOR PULSE 1ST!
|
HYPOVOLEMIA primary cause, treat like asystole,
|
|
|
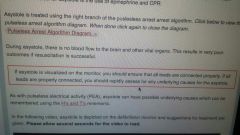
ASYSTOLE
|
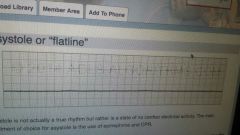
true state of NO Electrical Activity
|
|
|
|
1st ° AV Block
|
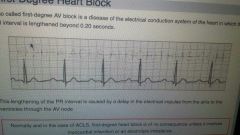
PR interval > 0.20 sec
|
of no consequence UNLESS MI or electrolyte imbalance
|
|
|
2nd ° Heart Block type 1
|
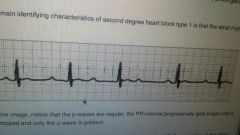
Also called Mobitz 1, PR interval prolonged till atrial impulse blocked, thus, no QRS impulse
|
Atrial rhythm will be REGULAR
|
|
|
2nd ° Heart Block type 2
|
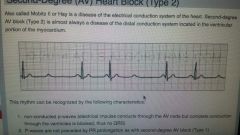
Mobitz II, almost always disease of distal/ventricular conduction
|
non conducted P waves, thus no QRS; no PR prolongation, wide QRS complex CAN LEAD TO COMPLETE BLOCK, txt= transcutaneous/transvenous pacing, or *Atropine
|
|
|
Complete Heart Block
|
3rd °, impulse generates in SA node, not conducted to ventricles
|
most common causes infarction & ischemia; txt= transcutaneous pacing; s&s= bradycardia, hypotension, hemodynamic instability
|
|
|
Supraventricular Tachycardia SVT
|
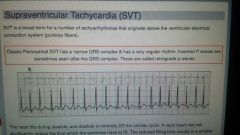
drop in cardiac output, HR >150 bpm
|
unstable, txt= cardioversion S&S= SOB, Palpitations, angina, dizziness, LOS, parasthesia, hyperventilation
|
|
|
Atrial Flutter
|
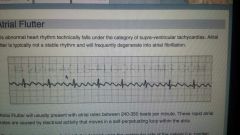
atrial contractions 240-350 bpm due to electrical activity in SA/AV node loop
|
S&S= palpitations, SOB,dizziness, nausea, impending doom, Peripheral edema, activity intolerance EARLY CARDIOVERSION
|
|
|
A FIB
|
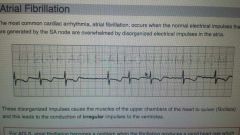
SA node overwhelmed by atrial impulses, leads to irregular impulses to ventricles
|
no P -waves before QRS, HR is IRREGULAR, same S&S as A flutter
|
|
|
Other Tachycardias
|
|
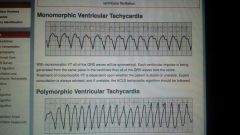
monomorphic will deteriorate to V-Fib; polymorphic originates in ventricles rather than normal rhythm (from atria)
|