Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
23 Cards in this Set
- Front
- Back
|
Antidepressants - Indications
|
Primary indication is Major depressive disorder
Post-partum depression Anxiety disorders Bulimia nervosa Pain Depression with medical illness Depression associated with schizophrenia |
|
|
General Considerations with the use of Antidepressants
|
Dosage
•Start with lowest dose and gradually increase •Abrupt cessation can lead to withdrawal Combination of drugs not recommended Suicide risk •Study showed increased suicide risk in persons taking antidepressants •Suicide by overdose may be attempted - 30% are treatment resistant Prevention of relapse •6 mths treatment to prevent relapse •Increased number of episodes increases the chance for more episodes |
|
|
Effects of Antidepressants
|
Do not produce euphoria
Have no discernible effects in non-depressed individuals (except MAO-Is) Have no reinforcing effects (ie: not likely to cause dependence) In depressed individuals they •elevate mood •increase physical activity •improve appetite and sleep patterns •reduce morbid preoccupation |
|
|
TCA Indications
|
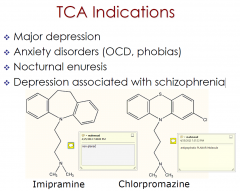
Major depression
Anxiety disorders (OCD, phobias) Nocturnal enuresis Depression associated with schizophrenia |
|
|
Tricyclic Antidepressants
|
Amitriptyline (Endep)
Clomipramine (Anafril, Placil) Dothiepin (Dothep, Prothiaden) Doxepin (Deptran, Sinequan) Imipramine (Melipramine) Nortriptyline (Allegron) Trimipramine (Surmontil |
|
|
TCA Pharmacology
|
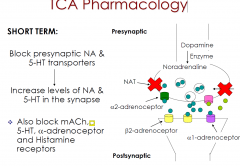
dirty drugs at therapeutic doses
- SE- seadtion - anticholinergic effects |
|
|
Overdose with TCAs
|
CNS
•Excitement, delirium, convulsions, drowsiness, respiratory depression, coma and death Cardiotoxicity •Cardiac depression •Arrhythmias •Hypotension TCAs strongly potentiate alcohol effects •Combination can cause death from respiratory depression Narrow TI - 1 weeks supply can be fatal |
|
|
MAOI Indications
|
Major depression
Major depression when other antidepressants have not worked (Phenelzine) Atypical depression Phobic anxiety & panic disorder Social phobia (Moclobemide) Anorexia and bulimia nervosa |
|
|
Monoamine Oxidase Inhibitors
|
Irreversible, non-selective: phenelzine, tranylcypromine
•Bind covalently to MAO-A and MAO-B Reversible Inhibitor of MAO-A (RIMA): moclobemide •Binds reversibly and selectively to MAO-A |
|
|
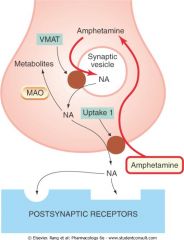
MAO MOA
|
|
|
|
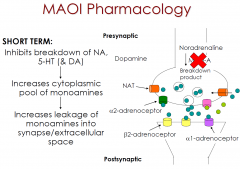
MAO Pharmacology
|
|
|
|
SSRI Indications
|
Major depression
Dysthymia Anxiety disorders (panic disorder, OCD) |
|
|
Selective Serotonin Reuptake Inhibitors
|
Citalopram (Celapram, Cipramil, Talam, Talohexal)
Escitalopram (Lexapro) Fluoxetine (Auscap, Fluohexal, Fluoxetine-DP, Fluoxebell, Lovan, Prozac, Zactin) Fluvoxamine (Faverin, Luvox, Movox) Paroxetine (Aropax, Oxetine, Paxtine) Sertraline (Xydep, Zoloft) |
|
|
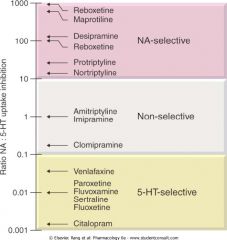
SSRI Relative Potency
|
|
|
|
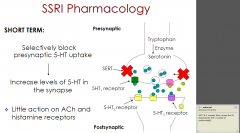
SSRI Pharmacology
|
|
|
|
Atypical Antidepressant Indications
|
Major depression
Prevention of relapse of major depression Anxiety disorders (GAD, social phobia) |
|
|
Atypical Antidepressants
|
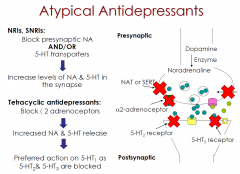
Tetracyclic antidepressants (a2-adrenoceptor blockers):
•Mianserin (Lumix) •Mirtazapine (Avanza, Axit, Mirtazon, Remeron) NRI: •Reboxetine (Edronax) SNRIs: •Venlafaxine (Efexor), Desvenlafaxine (Pristiq), Duloxetine (Cymbalta) |
|
|
Atypical Antidepressants Pharmacology
|
|
|
|
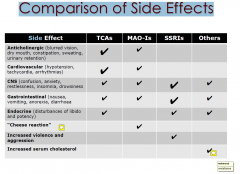
Comparison of Side Effects
Side |
|
|
|
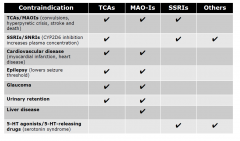
Contraindications
|
|
|
|
Long Term Effects of Antidepressants
|
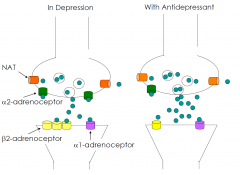
Over a period of a few weeks…
Down-regulate postsynaptic NA (-adreno-ceptors) and/or 5-HT2 receptors •Reduction in binding sites •Reduction in agonist response Increase activity/sensitivity of post-synaptic 5-HT1 receptors in hippocampus (except MAO-I’s) Decrease activity/sensitivity of presynaptic a2 adrenoceptors and/or 5-HT1 receptors (inhibitory receptors which control NA and 5-HT release) •Facilitate monoamine release Net effect of chronic treatment is an enhancement of monoaminergic function •optimize monoamine levels and restore optimal receptor sensitivity Slow adaptive changes correspond to the timecourse of therapeutic effect •β2 adrenoceptors downregulated •5-HT2 receptors downregulated •2 adrenoceptors downregulated |
|
|
Comparison of Efficacy
|
TCAs used as “gold standard” to measure antidepressant effects against
Newer drugs have reduced side/adverse effects, but not reduced number of “treatment resistant” persons MAOIs effective in atypical depression SSRIs very effective in reducing anxiety, agitation, retardation associated with depression. SSRIs as effective as TCAs in treating moderate depression, but possibly less effective than TCAs in treating severe depression |
|
|
A Question of Efficacy?
Kirsch et al (2008) meta-analysis: |
•symptom reduction among depressed patients on placebo ~30%; on antidepressants ~40%
•only 48% of approved antidepressants showed superiority over placebo •antidepressants only effective in severely depressed (as placebo less effective in this group) |