Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
128 Cards in this Set
- Front
- Back
|
What is a "leukemia"? Where are tumor cells?
|
- Lymphoid or myeloid neoplasm with widespread involvement of bone marrow
- Tumor cells are usually found in peripheral blood |
|
|
What is a "lymphoma"? Where are tumor cells?
|
- Discrete tumor mass arising from lymph nodes
- Presentations often blur definitions |
|
|
What is the term for an acute inflammatory response to infection?
|
Leukemoid Reaction
|
|
|
What causes a Leukemoid Reaction? What changes occur?
|
- Acute inflammatory response to infection
- ↑ WBC count with ↑ neutrophils and neutrophil precursors such as band cells (left shift) - ↑ Leukocyte ALP |
|
|
How does a Leukemoid Reaction compare to CML?
|
- Both have ↑ WBC count with ↑ neutrophils and neutrophil precursors such as band cells (left shift)
- Leukemoid Reaction has ↑ leukocyte ALP wherease CML has ↓ leukocyte ALP |
|
|
What are the types of lymphoma?
|
- Hodgkin
- Non-Hodgkin |
|
|
Which type of lymphoma has the following characteristics:
- Localized, single group of nodes - Extranodal involvement rare - Contiguous spread - Spread is strongest predictor of prognosis - Much better prognosis |
Hodgkin Lymphoma
|
|
|
Which type of lymphoma has the following characteristics:
- Multiple, peripheral noes - Extranodal involvement common - Non-contiguous spread - Worse prognosis |
Non-Hodgkin Lymphoma
|
|
|
What are the characteristics of nodal and extra-nodal involvement in Hodgkin Lymphoma?
|
- Localized, single group of nodes
- Extranodal involvement rare - Contiguous spread |
|
|
What are the characteristics of nodal and extra-nodal involvement in Non-Hodgkin Lymphoma?
|
- Multiple, peripheral noes
- Extranodal involvement common - Non-contiguous spread |
|
|
Which has a better prognosis Hodgkin vs Non-Hodgkin Lymphoma?
|
Hodgkin Lymphoma has a better prognosis
|
|
|
Which pathology is characterized by Reed-Sternberg cells?
|
Hodgkin Lymphoma
|
|
|
What kind of cells are typically affected in Non-Hodgkin Lymphoma?
|
- Majority involve B cells
- Exceptions: lymphoblastic T-cell origin |
|
|
Who is more commonly affected by Hodgkin vs Non-Hodgkin Lymphoma?
|
Hodgkin:
- Bimodal distribution: young adulthood and >55 years - More common in men, except for nodular sclerosing type Non-Hodgkin: - Peak incidence for certain subtypes at 20-40 years old |
|
|
What infection is associated with Hodgkin vs Non-Hodgkin Lymphoma? Other associations?
|
Hodgkin:
- 50% of cases associated with EBV Non-Hodgkin: - May be associated with HIV and immunosuppression |
|
|
What type of lymphoma is more so associated with the constitutional "B" signs/symptoms? What are they?
|
Hodgkin Lymphoma is more likely to have B signs:
- Low-grade fever - Night sweats - Weight loss Non-Hodgkin Lymphoma has fewer constitutional signs/symptoms |
|
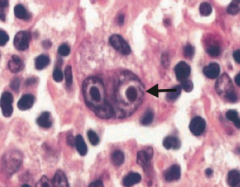
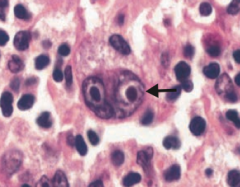
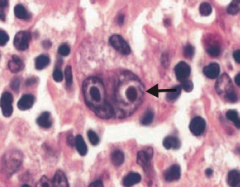
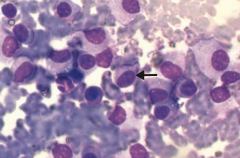
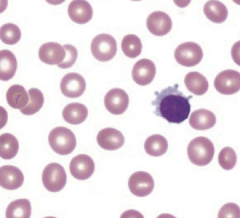
What is the arrow pointing to? Sign of?
|
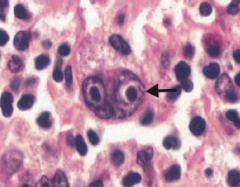
Reed-Sternberg cell
- Distinctive tumor giant cell seen in Hodgkin Lymphoma - Binucleate or bilobed with the 2 halves as mirror images ("owl eyes") |
|
|
What are the cell markers for Reed-Sternberg Cells? What kind of cells?
|
CD15+ and CD30+ B-cell origin
|
|
|
How does the presence of Reed-Sternberg Cells help you make a diagnosis?
|
Necessary but not sufficient for a diagnosis of Hodgkin Lymphoma
|
|
|
What characteristic of Hodgkin Lymphoma gives a better prognosis?
|
Better prognosis with strong stromal or lymphocytic reaction AGAINST Reed-Sternberg cells
|
|
|
What is the most common form of Hodgkin Lymphoma? Characteristics?
|
Nodular Sclerosing form
- Affects men and women equally |
|
|
Which types of Hodgkin Lymphoma have the best prognosis?
|
Lymphocyte-rich
|
|
|
Which types of Hodgkin Lymphoma have the poorest prognosis?
|
- Lymphocyte mixed
- Lymphocyte depleted |
|
|
What types of Non-Hodgkin Lymphomas are neoplasms of MATURE B cells?
|
- Burkitt Lymphoma
- Diffuse Large B-cell Lymphoma - Mantle Cell Lymphoma - Follicular Lymphoma |
|
|
What types of Non-Hodgkin Lymphomas are neoplasms of MATURE T cells?
|
- Adult T-cell Lymphoma
- Mycosis Fungoides / Sézary Syndrome |
|
|
Who is typically affected by the types of NHL of mature B cells?
|
- Burkitt Lymphoma: adolescents or young adults
- Diffuse Large B-cell Lymphoma: usually older adults (but 20% in children) - Mantle Cell Lymphoma: older males - Follicular Lymphoma: adults |
|
|
What genetic change is associated with Burkitt Lymphoma?
|
t(8;14) translocation of c-myc (8) and heavy-chain Ig (14)
|
|
|
What genetic change is associated with Diffuse Large B-cell Lymphoma?
|
t(14;18)
|
|
|
What genetic change is associated with Mantle Cell Lymphoma?
|
t(11;14) - translocation of cyclin D1 (11) and heavy chain Ig (14)
|
|
|
What genetic change is associated with Follicular Lymphoma?
|
t(14;18) - translocation of heavy chain Ig (14) and bcl-2 (18)
|
|
|
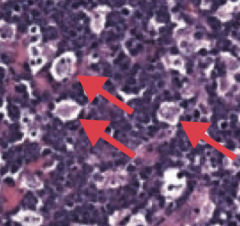
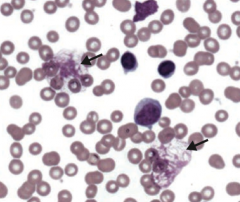
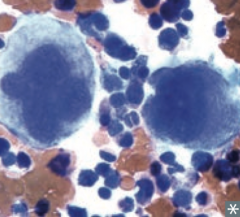
What neoplasm is associated with the t(8;14) translocation? Classic histologic appearance?
|
Burkitt Lymphoma
- Associated with "starry sky" appearance: sheets of lymphocytes with interspersed macrophages (arrows/stars) |
|
|
What is Burkitt Lymphoma associated with?
|

- Associated with EBV
- Jaw lesions in endemic form in Africa - Pelvis or abdomen tumors in sporadic form |
|
|
What is the most common type of non-Hodgkin Lymphoma in adults? Translocation?
|
Diffuse Large B-cell Lymphoma - t(14;18)
|
|
|
What neoplasm is associated with the t(11;14) translocation? Who is classically affected by this?
|
Mantle Cell Lymphoma
- Classically in older males |
|
|
What type of neoplasm is associated with being CD5+? Genetics?
|
Mantle Cell Lymphoma
- t(11;14) - translocation of cyclin D1 (11) and heavy chain Ig (14) |
|
|
What neoplasm is associated with the t(14;18) translocation? Who is classically affected by this?
|
Follicular Lymphoma
- Typically affects adults |
|
|
What is the effect of the translocation in Follicular Lymphoma?
|
t(14;18) - translocation of heavy chain Ig (14) and bcl-2 (18)
- bcl-2 is up-regulated and inhibits apoptosis |
|
|
How does Follicular Lympoma present? Course?
|
- Presents with painless "waxing and waning" lymphadenopathy
- Indolent course |
|
|
What neoplasm is caused by HTLV-1? What is this virus associated with?
|
Adult T-cell Lymphoma
- HTLV-1 is associated with IV drug abuse |
|
|
Who is more likely to get Adult T-cell Lymphoma? How does it present?
|
- More common in adults, especially those from Japan, West Africa, and the Caribbean
- Presents with cutaneous lesions, lytic bone lesions, and hypercalcemia |
|

What lymphoma presents with cutaneous patches / plaques / tumors? What kind of cells?
|

Mycosis Fungoides
- Mature T cells (CD4+) |
|
|
What is the characteristic finding of Sézary Syndrome?
|

Similar to Mycosis Fungoides (cutaneous patches / plaques / tumors) with circulating malignant cells seen in Sézary Syndrome
|
|
|
What is the course of Mycosis Fungoides / Sézary Syndrome?
|
- There is potential to spread to lymph nodes and viscera
- Indolent |
|
|
Which type of neoplasm is associated with hypercalcemia, renal insufficiency, anemia, bone lytic lesions, and back pain? What cells are affected?
|
Multiple Myeloma
- Monoclonal plasma cell cancer Symptoms - think CRAB: - Hypercalcemia - Renal insufficiency - Anemia - Bone lytic lesions / Back pain |
|
|
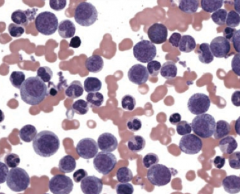
What is the histologic appearance in Multiple Myeloma?
|
Monoclonal plasma cells look like "fried eggs" due to large eccentric nuclei
|
|
|
What is the most common primary tumor arising within the bones of the elderly (>40-50 years)?
|
Multiple Myeloma
|
|
|
What is wrong in Multiple Myeloma?
|
- Monoclonal plasma cell cancer
- Arises in BM and produces large amounts of IgG (55%) or IgA (25%) |
|
|
What is Multiple Myeloma associated with?
|
- ↑ Susceptibility to infection
- Primary amyloidosis (AL) - Punched out lytic bone lesions on x-ray - M spike on serum protein electrophoresis - Ig light chains in urine (Bence Jones protein) - Rouleaux formation (RBCs stacked like poker chips in blood smear) |
|
|
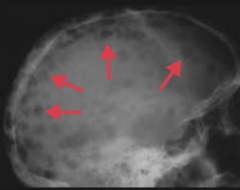
What is the appearance of Multiple Myeloma on x-ray?
|
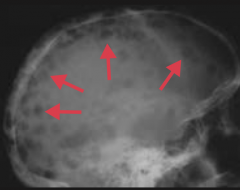
Punched-out lytic bone lesions
|
|
|
What is the typical lab finding indicative of Multiple Myeloma?
|
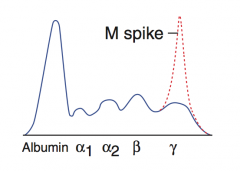
M spike on serum protein electrophoresis (indicating monoclonal Ab production)
|
|
|
What is the classic urine finding in Multiple Myeloma?
|
Ig light chains in urine = Bence Jones proteins
|
|
|
What are Bence Jones proteins? Finding of?
|
Ig light chains in urine = sign of Multiple Myeloma
|
|
|
What is the appearance of Multiple Myeloma on blood smear?
|
- Rouleaux formation (RBCs stacked like poker chips)
- Plasma cells with eccentric nuclei (looks like a fried egg) - Numerous plasma cells with "clock face" chromatin and intracytoplasmic inclusions containing imunoglobulin |
|
|
What diagnosis do you need to distinguish Multiple Myeloma from?
|
Waldenström Macroglobulinemia → M spike = IgM (→ hyperviscosity symptoms)
- WM has no lytic bone lesions |
|
|
What kind of antibodies are elevated in Multiple Myeloma?
|
- IgG (55% of cases)
- IgA (25% of cases) |
|
|
What is the diagnosis if there is a monoclonal expansion of plasma cells with serum monoclonal protein <3g/dL ("M spike") and BM with <10% monoclonal plasma cell?
|
Monoclonal Gammopathy of Undetermined Significance (MGUS)
- Asymptomatic precursor to Multiple Myeloma - Patients with MGUS develop Multiple Myeloma at a rate of 1-2% per year (so must follow up with these patients) |
|
|
What are the characteristics of Monoclonal Gammopathy of Undetermined Significance (MGUS)?
|
- Monoclonal expansion of plasma cells with serum monoclonal protein <3g/dL ("M spike")
- BM with <10% monoclonal plasma cell - Asymptomatic precursor to Multiple Myeloma - Patients with MGUS develop Multiple Myeloma at a rate of 1-2% per year (so must follow up with these patients) |
|
|
What kind of disorders are myelodysplastic syndromes? What is wrong?
|
Stem cell disorders involving ineffective hematopoiesis → defects in cell maturation of all non-lymphoid lineages
|
|
|
What causes Myelodysplastic Syndromes?
|
De novo mutations or environmental exposure (eg, radiation, benzene, chemotherapy)
|
|
|
What can Myelodysplastic Syndromes transform to?
|
AML
|
|
|
What is it called when neutrophils become bilobed after chemotherapy?
|
Pseudo-Pelger Huet anomaly
|
|
|
What is the Pseudo-Pelger Huet anomaly?
|
Neutrophils with bilobed nuclei (two nuclear masses connected with a thin filament of chromatin) typically seen after chemotherapy
|
|
|
What is wrong in a leukemia?
|
- Unregulated growth of leukocytes in BM
- ↑ or ↓ numbers of circulating leukocytes in blood and marrow failure |
|
|
What are the potential complications of a leukemia?
|
- Leads to anemia (↓ RBCs), infections (↓ mature WBCs), and hemorrhage (↓ platelets)
- Leukemic cell infiltrate of the liver, spleen, and lymph nodes, is possible |
|
|
What are the types of lymphoid leukemias?
|
- Acute lymphoblastic leukemia / lymphoma (ALL)
- Small lymphocytic lymphoma (SLL) / Chronic lymphocytic leukemia (CLL) - Hairy cell leukemia |
|
|
What are the types of myeloid leukemias?
|
- Acute myelogenous leukemia (AML)
- Chronic myelogenous leukemia (CML) |
|
|
Which lymphoid leukemia is most common in those under 15 years?
|
Acute Lymphoblastic Leukemia / Lymphoma (ALL)
|
|
|
What is the most common location of a mass in Acute Lymphoblastic Leukemia / Lymphoma (ALL)? Why that location?
|
Mediastinal mass (leukemic infiltration of the thymus)
|
|
|
Which type of leukemia is associated with Down Syndrome?
|
- Acute Lymphoblastic Leukemia / Lymphoma (ALL)
- Acute Myelogenous Leukemia (AML) |
|
|
What are the lab findings in Acute Lymphoblastic Leukemia / Lymphoma (ALL)?
|
- Peripheral blood and bone marrow have ↑↑↑ lymphoblasts
- TdT+ (marker of pre-T and pre-B cells) - CD10+ (pre-B cells only) |
|
|
Where can Acute Lymphoblastic Leukemia / Lymphoma (ALL) spread to? Prognosis?
|
- Can spread to CNS and testes
- Most responsive to therapy - t(12;21) → better prognosis |
|
|
Which type of leukemia is CD2+ and CD5+? What kind of cells?
|
Small Lymphocytic Lymphoma (SLL) / Chronic Lymphocytic Leukemia (CLL)
- B cell neoplasm |
|
|
What is the histologic appearance of Small Lymphocytic Lymphoma (SLL) / Chronic Lymphocytic Leukemia (CLL)?
|
- Smudge cells in periphreal blood smear
- Auto-immune hemolytic anemia |
|
|
What is the prognosis / course of Small Lymphocytic Lymphoma (SLL) / Chronic Lymphocytic Leukemia (CLL)?
|
Often asymptomatic, progresses slowly
|
|
|
What is the difference between Small Lymphocytic Lymphoma (SLL) and Chronic Lymphocytic Leukemia (CLL)?
|
SLL is the same as CLL except that CLL has ↑ peripheral blood lymphocytosis or bone marrow involvement
|
|
|
What is the histologic appearance of Hairy Cell Leukemia? What kind of cells are affected?
|
- Mature B-cell tumor
- Cells have filamentous, hair-like projections |
|
|
Who is the typical patient to get the different types of lymphoid leukemias?
|
- ALL: <15 years
- SLL/CLL: >60 years - Hairy Cell Leukemia: adults |
|
|
How can you confirm a diagnosis of Hairy Cell Leukemia?
|
Stains TRAP (tartate-resistant acid phosphatase (+))
- TRAP stain largely replaced now with flow cytometry Causes marrow fibrosis → dry tap on aspiration Hairy Cell - think TRAP and TAP (dry) |
|
|
How do you treat Hairy Cell Leukemia?
|
Cladribine (2-CDA), an adenosine analog (resistant to adenosine deaminase)
|
|
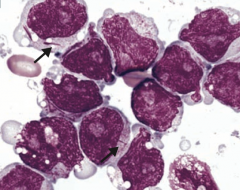
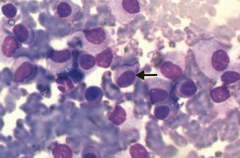
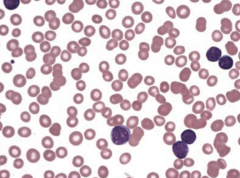
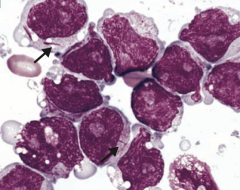
What kind of cells are these? What type of disease?
|
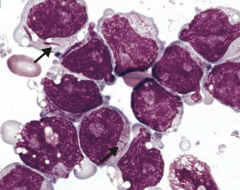
- Myeloblasts containing Auer rods
- Seen in Acute Myelogenous Leukemia (AML) |
|
|
What are the blood smear findings associated with Acute Myelogenous Leukemia (AML)?
|
- Auer rods
- Peroxidase (+) cytoplasmic inclusions seen mostly in M3 AML - ↑↑↑ circulating myeloblasts |
|
|
When does Acute Myelogenous Leukemia (AML) typically occur? What are the risk factors for it?
|
- Median age of onset 65 years
Risk factors: - Prior exposure to alkylating agent chemotherapy - Exposure to radiation - Myeloproliferative disorders - Down Syndrome |
|
|
What genetic change is associated with M3 AML? Other characteristics of this subtype?
|
t(15;17)
- Responds to all-trans retinoic acid (ATRA / vitamin A) - ATRA induces differentiation of myeloblasts - DIC is a common presentation in M3 AML |
|
|
What is the mechanism of all-trans retinoic acid (ATRA)? What is it used for?
|
- Induces differentiation of myeloblasts
- Used for the t(15;17) M3 subtype of AML |
|
|
What type of leukemia is associated with DIC?
|
M3 AML t(15;17)
|
|
|
What genetic change is associated with Chronic Myelogenous Leukemia (CML)?
|
Philadelphia chromosome t(9;22) - bcr-abl (tyrosine kinase)
|
|
|
When is Chronic Myelogenous Leukemia (CML) more common?
|
Peak incidence 45-85 years, median age at diagnosis 64 years
|
|
|
What changes occur in Chronic Myelogenous Leukemia (CML)?
|
- Myeloid stem cell proliferation
- Presents with ↑ neutrophils, metamyelocytes, and basophils - Splenomegaly |
|
|
What can Chronic Myelogenous Leukemia (CML) lead to?
|
May accelerate and transform to AML or ALL ("blast crisis")
|
|
|
What lab finding is associated with Chronic Myelogenous Leukemia (CML) vs Leukemoid Reaction?
|
- CML: very low leukocyte Alkaline Phosphatase
- Leukemoid reaction: increased leukocyte Alkaline Phosphatase |
|
|
How can you treat Chronic Myelogenous Leukemia (CML)? Mechanism?
|
Imatinib - a small-molecule inhibitor of the bcr-abl tyrosine kinase
|
|
|
What disorder is associated with t(9;22)?
|
This is the Philadelphia chromosome = CML (bcr-abl hybrid)
|
|
|
What disorder is associated with t(8;14)?
|
Burkitt lymphoma (c-myc activation)
|
|
|
What disorder is associated with t(11;14)?
|
Mantle cell lymphoma (cyclin D1 activation)
|
|
|
What disorder is associated with t(14;18)?
|
Follicular lymphoma (bcl-2 activation)
|
|
|
What disorder is associated with t(15;17)?
|
M3 type of AML (responsive to all-trans retinoic acid)
|
|
|
What is the name of the proliferative disorder of the dendritic cells? Lineage?
|
Langerhans cell Histiocytosis - monocyte lineage
|
|
|
What diagnosis should you consider in a child presenting with lytic bone lesions and a skin rash, or as recurrent otitis media with a mass involving the mastoid bone?
|
Langerhans cell Histiocytosis - proliferative disorder of dendritic (Langerhans) cells from monocyte lineage
|
|
|
What is the classic presentation of Langerhans cell Histiocytosis?
|
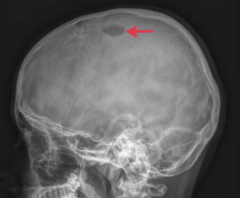
- In a child with lytic bone lesions (picture) and skin rash
- In a child with recurrent otitis media with a mass involving the mastoid bone |
|
|
What is wrong with the cells in Langerhans cell Histiocytosis?
|
Cells are functionally immature and do not efficiently stimulate primary T lymphocytes via antigen presentation
|
|
|
What are the typical lab findings of Langerhans cell Histiocytosis?
|

- Cells express S-100 (mesodermal origin) and CD1a
- Birbeck granules ("tennis rackets" on EM) are characteristic |
|
|
What does it mean if a cell expresses S-100?
|
Cell is of mesodermal origin (this is true in Langerhans cell Histiocytosis of the dendritic cells)
|
|
|
What do the cells in Langerhans cell Histiocytosis express?
|
- S-100 (mesodermal origin)
- CD1a |
|

What is this finding suggestive of?
|

These are Birbeck Granules (tennis rackets) → Langerhans cell Histiocytosis
|
|
|
What are the types of Chronic Myeloproliferative Disorders?
|
- Polycythemia Vera
- Essential Thrombocytosis - Myelofibrosis - CML |
|
|
What gene is involved in hematopoietic growth factor signaling?
|
JAK2
|
|
|
What is the diagnosis in a patient with a hematocrit >55% with a somatic mutation in the JAK2 gene?
|
Polycythemia Vera
|
|
|
What diagnosis should you consider in a patient that has intense itching after a hot shower? What should you look at to confirm?
|
Polycythemia Vera
- Hematocrit will be >55% - Somatic mutation in JAK2 gene |
|
|
What is the rare, but classic, symptom in Polycythemia Vera?
|

Erythromelalgia - severe, burning pain and reddish or bluish discoloration due to episodic blood clots in vessels of the extremities
|
|
|
What is Erythromelalgia? What does it indicate?
|

- Severe, burning pain and reddish or bluish discoloration due to episodic blood clots in vessels of the extremities
- Rare but classic symptom of Polycythemia Vera |
|
|
What can cause secondary polycythemia?
|
Natural or artificial increase in EPO levels
|
|
|
What disorder is similar to polycythemia vera but is specific for overproduction of abnormal platelets? Symptoms?
|
Essential Thrombocytosis
- Bleeding - Thrombosis |
|
|
What blood smear finding is associated with Essential Thrombocytosis?
|
Enlarged megakaryocytes → overproduction of abnormal platelets → bleeding, thrombosis
|
|
|
What is wrong in Myelofibrosis?
|
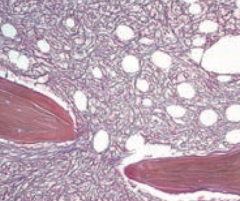
Fibrotic obliteration of bone marrow
|
|
|
What peripheral blood smear finding is associated with Myelofibrosis?
|
Teardrop RBCs and immature forms of the myeloid line
"Bone marrow is crying because it's fibrosed" |
|
|
What diagnosis should you think of if you see teardrop RBCs on peripheral blood smear? How do you confirm?
|
Myelofibrosis - look at bone marrow - should be fibrotic obliteration and there should also be immature forms of the myeloid lineage
|
|
|
What myeloproliferative disorder has:
- RBCs: ↑ - WBCs: ↑ - Platelets: ↑ - JAK2 mutation |
Polycythemia Vera
|
|
|
What myeloproliferative disorder has:
- RBCs: - - WBCs: - - Platelets: ↑ - JAK2 mutation (30-50%) |
Essential Thrombocytosis
|
|
|
What myeloproliferative disorder has:
- RBCs: ↓ - WBCs: Variable - Platelets: Variable - JAK2 mutation (30-50%) |
Myelofibrosis
|
|
|
What myeloproliferative disorder has:
- RBCs: ↓ - WBCs: ↑ - Platelets: ↑ - Philadelphia chromosome |
CML
|
|
|
How are the following affected by ↓ plasma volume (dehydration, burns)?
- Type of polycythemia: - Plasma Volume: - RBC mass: - O2 saturation: - EPO levels: |
Relative Polycythemia
- Plasma Volume: ↓ - RBC mass: - - O2 saturation: - - EPO levels: - |
|
|
How are the following affected by lung disease, congenital heart disease, or high altitude?
- Type of polycythemia: - Plasma Volume: - RBC mass: - O2 saturation: - EPO levels: |
Appropriate Absolute Polycythemia:
- Plasma Volume: - - RBC mass: ↑ - O2 saturation: ↓ - EPO levels: ↑ |
|
|
How are the following affected by renal cell carcinoma, Wilms tumor, cyst, hepatocellular carcinoma, hydronephrosis?
- Type of polycythemia: - Plasma Volume: - RBC mass: - O2 saturation: - EPO levels: |
Inappropriate Absolute Polycythemia (due to ectopic EPO)
- Plasma Volume: - - RBC mass: ↑ - O2 saturation: - - EPO levels: ↑ |
|
|
How are the following affected by polycythemia vera?
- Plasma Volume: - RBC mass: - O2 saturation: - EPO levels: |
- Plasma Volume: ↑
- RBC mass: ↑↑ - O2 saturation: - - EPO levels: ↓ (due to negative feedback) |
|
|
The following findings can be caused by what?
- Plasma Volume: ↓ - RBC mass: - - O2 saturation: - - EPO levels: - |
↓ Plasma volume (dehydration or burns) = Relative Polycythemia
|
|
|
The following findings can be caused by what?
- Plasma Volume: - - RBC mass: ↑ - O2 saturation: ↓ - EPO levels: ↑ |
Lung disease, congenital heart disease, high altitude = Appropriate Absolute Polycythemia
|
|
|
The following findings can be caused by what?
- Plasma Volume: - - RBC mass: ↑ - O2 saturation: - - EPO levels: ↑ |
Renal cell carcinoma, Wilms tumor, cyst, hepatocellular carcinoma, hydronephrosis
Inappropriate absolute polycythemia (due to ectopic EPO) |
|
|
The following findings can be caused by what?
- Plasma Volume: ↑ - RBC mass: ↑↑ - O2 saturation: - - EPO levels: ↓ |
Polycythemia Vera = due to negative feedback
|