Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
29 Cards in this Set
- Front
- Back
|
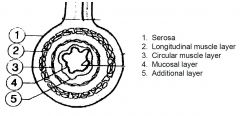
Structure of the GI tract wall
|
|
|
|
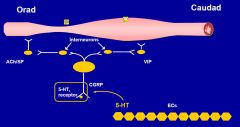
INNERVATIONAND CONTROL OF MOTILITY
- step 1 |
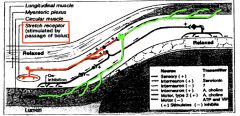
Stretch receptors in myentericplexus (between the circular and longitudinal muscle layers) sense the passage of a bolus and stimulate neuronesto release an unknown NT which stimulate serotonergicinterneuroneswhich then stimulate motor neuronesto release AChand cause circular muscle contraction
|
|
|
INNERVATIONAND CONTROL OF MOTILITY
- step 2 |
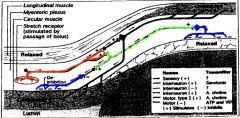
Stretch receptors also cause activation of Cholinergic interneuroneswhich in turn stimulate inhibitory neuronesto cause relaxation of circular muscle in front of the bolus and also behind the stretch receptors
|
|
|
Define the term GI motility
|
•Definition:
the spontaneous movements of the digestive tube, encompassing Contractile activity / tone Flow / transit Compliance |
|
|
Describe four general functions of motility
|
•Propulsion
•Storage •Mixing –Mechanical dispersion –Contact with digestive secretions –Contact with absorptive cells •Prevention of retrograde movement of contents to proximal organs –sphincters |
|
|
Discuss motor functions of different gut regions
|
- propulsion
- sotrage - mixing - usually more than one function to an area - all have propulsion |
|
|
List techniques to measure gut motility
|
•Radiography/fluoroscopy
•Scintigraphy •Manometry •Barostat |
|
|
Describe major patterns of GI motility
|
- oesophagus
|
|
|
Describe the neural control of gut motility
|
•Most activity of GI tract takes place without perception
•mouth, UOS and striated muscle of proximal oesophagus and anus - only conscious influence •other activities of gut proceed automatically and are controlled by autonomic NS and a network of cells in gut wall called the enteric nervous system (ENS) - ACTS LIKE A BRAIN |
|
|
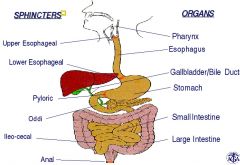
Sphincters
|
|
|
|
Major patterns of digestive tract motility
•oesophagus: |
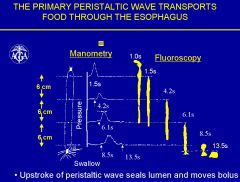
–primary peristalsis: response to swallowing
–secondary peristalsis: response to clear oesophagus |
|
|
Major patterns of digestive tract motility
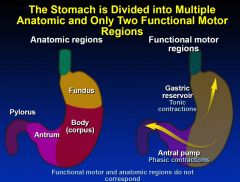
•stomach: |
–proximal stomach: tonic receptive relaxation to accommodate food- „reservoir‟; subsequent tonic contraction to facilitate emptying
–distal stomach: phasic antral contractions grind and empty contents (0.5-1.5mm)- „antral pump‟ 0.5-1.5 thus things can get stuck (eg chewing gum) |
|
|
The Stomach is Divided into Multiple Anatomic and Only Two Functional Motor Regions
|
|
|
|
Motility in Small Bowel
|
•small bowel:
–interdigestive motor activity (migrating motor complex) –digestive motor pattern (irregular mixing contractions) |
|
|
MMC
|
rapid sequece in response to (fast irregular contraction, lumenal excluding contractions to clear the whole bowel, sweeping down th e bowel, and itgets sloer and sloer and longer and longer as it goes thorugh the bowel (it occurs spontaneusly in the stomach called the stomach brain thing)
|
|
|
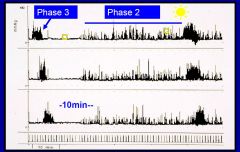
Interdigestive (fasting) motility of the
small bowel Phase 1, 2, 3 |
|
|
|
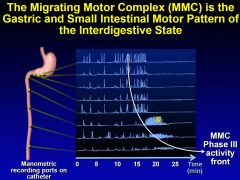
The Migrating Motor Complex Occurs Periodically in the Interdigestive State in the Stomach and Small Intestine
|

while we sleep our body is actively sweeping and clearing
|
|
|
Motility in Colon & ano-rectum:
|
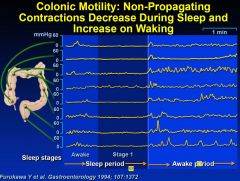
–phasic & tonic contractions (mixing, propulsion)
–gastro-colic reflex: increased contractile activity after eating –defaecation |
|
|
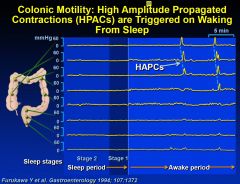
HPACs
|
|
|
|
Scintigraphic colonic transit
|
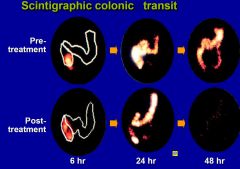
pre and post constipation Tx
|
|
|
What happens when we are fasting?
|
•Small intestine almost empty
•Migrating motor complex (MMC) in stomach –phase I: stomach quiescent –phase II: peristaltic contractions resume –phase III: increase force of contractions, indigestible solid leaves stomach (>1.5mm), contents swept to ileum in 1.5 hours •MMC in small bowel -“housekeeper” : prevent stasis and bacterial overgrowth; three phases |
|
|
What happens when we eat?
|
•relaxation proximal stomach
•regular peristaltic contractions in stomach •irregular small intestinal contractions •increase in colonic phasic contractions •increase in colonic tone (30%) |
|
|
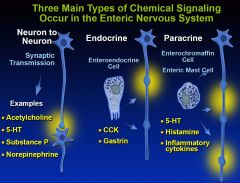
Enteric nervous system
|
•Controls motility and secretory functions of the intestine
•Semi-autonomous - actions modified by parasympathetic & sympathetic nervous systems - may function independently |
|
|
Three Main Types of Chemical Signaling Occur in the Enteric Nervous System
|
|
|
|
The peristaltic reflex
|
|
|
|
Autonomic control
•Parasympathetic (PSNS) |
–vagus nerve : oesophagus - ascending colon; vagus also has afferent fibres
–sacral spinal cord : pelvic splanchnic nerves - distal colon and rectum –most important neurotransmitter is acetylcholine (Ach) |
|
|
Autonomic control
•Sympathetic |
–thoracolumbar spinal cord : sympathetic ganglia e.g. coeliac ganglia, and synapse with postganglionic nerve cells whose fibres follow mesenteric vessels and end in intramural plexus
–most important neurotransmitter is noradrenaline –also afferents: distension, ischaemia, mucosal damage |
|
|
ENS vs Autonomic innervation
|
•Isolated stomach has peristalsis! ENS
•Fasting: complex pattern, MMC cycling controlled by ENS •Sight/chewing of food: vagus - gastric acid •Accommodation of proximal stomach - vagus •Fed pattern: vagus •Tonic inhibition - sympathetic |
|
|
Symptoms of GI tract dysmotility
|
•Oesophagus - heartburn, dysphagia, regurgitation, chest pain
•Stomach - dyspepsia, nausea, vomiting, anorexia, early satiety •Small intestine - abdominal pain, bloating, abdominal distention •Colon - abdominal pain,diarrhoea, constipation •Anorectum - urgency, incomplete evacuation, incontinence, straining |