![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
132 Cards in this Set
- Front
- Back
|
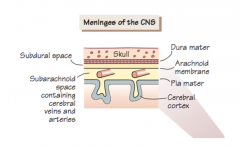
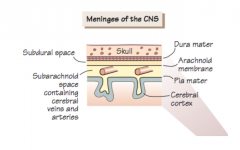
Draw the layers of the meninges |
|
|
|
What is the epidural space and where is it located. |
Space between the dura mater and the bone. In the brain: potential space (dura touches skull) In the spinal cord: anatomical space |
|
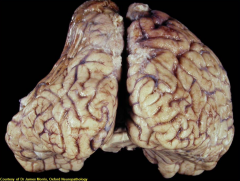
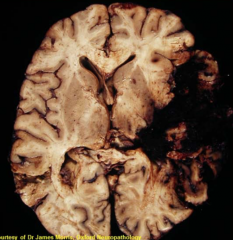
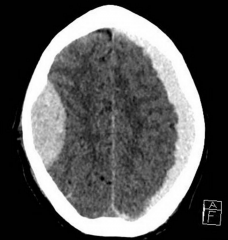
What intracranial haemorrhage can cause this morphology? |
Chronic subdural haemorrhage since there is no midline shift |
|
Describe the pathology |
Subfalcine herniation |
|
|
A patient suffers significant trauma to the right side of the head and is found to be paralysed on the right side (ipsilateral hemiplegia). What is the likely course of action? |
Acute trauma ⇒ Acutely increased ICP ⇒ Kernohan's notch (compression of the contralateral midbrain cerebral peduncle containing CoST) |
|
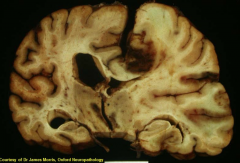
What is the pathology: A. Subdural haemorrhage B. Extradural haemorrhage C. Infarction |
Infarction because the underlying structure is still visible |
|
|
Glasgow Coma Scale |
Eye opening: 1-4 Verbal: 1-5 Motor response: 1-6 Min: 3/15 Max: 15/15 |
|
|
What part of the brain needs to be lesioned to cause structural coma? |
A. Reticular activating system (floor of 4th ventricle, peri-acqueductal grey and posterior thalamus) B. Severe damage to both hemispheres |
|
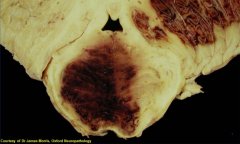
What is the pathology? |
Burst lobe: contusion extending to subdural space |
|
|
What distinguishes contusion from laceration? |
Pia-arachnoid membranes are torn over the site of injury in laceration |
|
|
Histology of diffuse axonal injury |

Swollen axons and axonal retraction bulbs due to shearing forces |
|
|
Diagnosis of diffuse axonal injury |
Histology ⇒ Swollen axons and axonal retraction bulbs due to shearing forces |
|
|
Two complications of diffuse axonal injury |
Loss of consciousness Risk of diffuse brain swelling |
|
|
Patient presents with progressive decline in GCS. He had undergone head injury while playing cricket and lost consciousness at that time but then awoke and felt relatively normal for a couple of hours. Likely diagnosis? How should the pt be managed? Possible complication? |
Extradural haematoma = Epidural haemorrhage Emergency evacuation of the haematoma Complication: Herniation |
|
|
Pathophysiology of extradural haematoma |
Arterial rupture (typically: middle meningeal artery) |
|
|
What blood vessels cause haemorrhage in: Extradural haemorrhage (EDH) Subdural haemorrhage (SDH) |

EDH: Arterial rupture (typically: middle meningeal artery) Acute SDH: Venous sinus rupture or small bridging veins rupture Chronic SDH: Small bridging veins rupture |
|
|
Presentation of acute SDH |
Rapid onset of raised ICP |
|
|
Presentation of chronic SDH |
Personality change, memory loss ➙ No midline shift |
|
|
Management of subdural haemorrhage (SDH) |
Acute (blood is clotted): Invasive emergency evacuation Chronic (blood is liquid): Burr hole evacuation |
|
|
Name the three types of cerebral oedema and their pathophysiology |
Vasogenic Damage to the BBB Cytotoxic Influx of cations and water into cells due to membrane damage or energy depletion (ion pumps fail) Interstitial Damage to ependymal lining in hydrocephalus or osmotic imbalance |
|
|
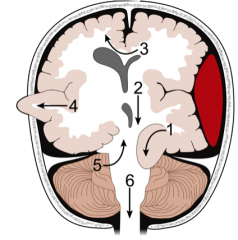
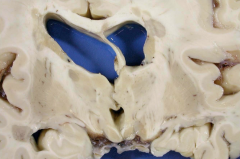
1 - Transtentorial herniation (= uncal herniation) 2 - Central herniation 3 - Subfalcine herniation 4 - Transcalvarial herniation 5 - Upward herniation 6 - Tonsillar herniation (= transforaminal herniation) |
|
|
One specific complication pertaining to bone injuries |
Fat embolism |
|
|
Diagnosis of brain death (and differential) |
Positive diagnosis of structural lesion Coma Loss of brainstem reflexes No spontaneous respiration Differential: Hypothermia, drug intoxication, metabolic/endocrine dysfunction |
|
|
What is the most likely cause of stroke among the following? Justify your answer. A. Atherosclerosis in the circle of Willis B. Atheroembolism from the origin of the internal carotid artery C. Atherosclerosis of the external carotid artery D. Haemorrhage of a major artery due to hypertension E. DVT-derived embolism F. Paradoxical cardiac embolus G. Mural thrombus in the heart secondary to MI |
A, B, D, F and G all can all cause a stroke theoretically. B, D, F, G are most common and B is the most common. A. Can cause stroke but typically there is some functional reserve due to redundancy B. Most likely C. External carotid only supplies blood to the face and neck. Furthermore these are large arteries are unlikely to be obstructed by atherosclerosis. D. Haemorrhagic stroke is 9x less likely than ischaemic stroke E. Embolus from DVT could not travel to the brain except in paradoxical embolus F. Can cause stroke but is less likely G. Can cause stroke but is less likely |
|
|
Commonest site for infarction |
Territory of middle cerebral artery (or some of its branches) |
|
Likely cause |
Ischaemic stroke of MCA |
|
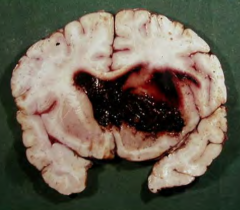
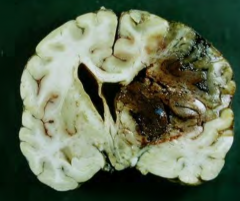
Likely cause |
Haemorrhagic stroke of the basal ganglia that has ruptured into the ventricles |
|
|
Three risk factors for stroke |
Diabetes, smoking, hypertension (Hypertension is #1 for haemorrhagic stroke) |
|
|
Post mortem brain histology reveals eosinophilic (red) neurons. Name a possible diagnosis. Is it possible to be the cause of death? |
Ischaemic stroke 1-4/7 ago ⇒ Possible
|
|
|
Post mortem brain histology reveals a cyst formed surrounded by gliosis and small number of persistent foamy Mϕ. Name a possible diagnosis. Is it possible to be the cause of death? |
Old ischaemic stroke 1/12-12/12 ago ⇒ Probably not the cause of death |
|
|
What do people die of in ischaemic stroke? |
Acute: Brain swelling (mostly oedema) ➙ Downward pressure ➙ Brain stem compression Later: Complications (pneumonia, pulmonary emboli) |
|
|
Histological presentation of ischaemic stroke |
0-24h – Oedema (early) 1d-4d – Eosinophilic (red) neurons 5-12d – Endothelial proliferation and neovascularisation 5-30d – Nϕ infiltration and microglial activation 8-14d – Foamy Mϕ infiltration, gliosis >50d – Cyst formed surrounded by gliosis and small number of persistent foamy Mϕ |
|
|
What are lacunar infarcts |
Atheroma at the base of small penetrating vessels ⇒ Small infarcts in deep GM/WM very common in elderly |
|
|
What are watershed infarcts |
Global hypoperfusion or hypoxia ⇒ Bilateral infarcts at junctions between arterial territories |
|
|
What is the pathophysiology of venous infarction? What is the two principal aetiologies and how do they present macroscopically? |

|
|
|
Most common site of haemorrhagic stroke |
Basal ganglia/Internal capsule (b.c. large high flow vessels directly give rise to small ones) |
|
|
Pathogenesis of haemorrhagic stroke (most commonly) |
A. Hypertension ⇒ Charcot-Bouchard microaneurysms in small blood vessels ⇒ Rupture B. Rupture of berry aneurysm |
|
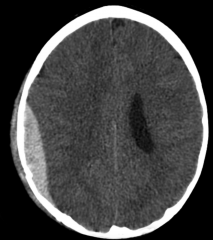
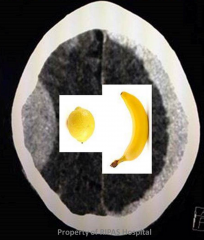
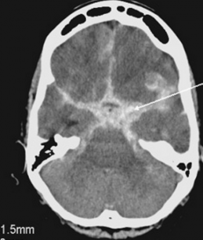
Likely diagnosis? |
Subdural haemorrhage
Compression of the brain but no infiltration in sucli and fissures and banana-shaped |
|

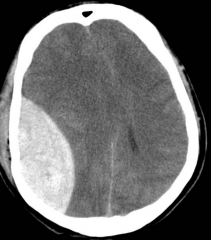
Likely diagnosis? |
Subdural haemorrhage Compression of the brain but no infiltration in sucli and fissures and banana shaped |
|
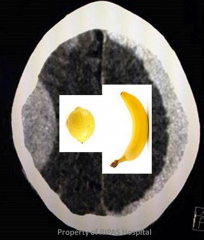
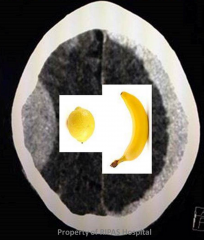
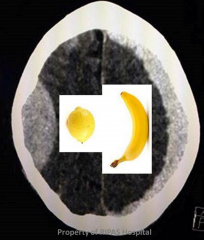
Likely diagnosis? |
Subdural and extradural haemorrhage Compression of the brain but no infiltration in sucli and fissures and banana shaped (right) and lemon shaped (left) |
|
Likely diagnosis? |
Extradural haemorrhage Compression of the brain but no infiltration in sulci and fissures and lemon shaped |
|

Likely diagnosis? |
Subarachnoid haemorrhage No compression of the brain but infiltration of blood in sulci, fissures and brainstem |
|
Likely diagnosis? |
Subarachnoid haemorrhage No compression of the brain but infiltration of blood in sulci, fissures and brainstem |
|
|
Two congenital causes of hydrocephalus |
Cerebral aqueduct stenosis Cerebral aqueduct atresia |
|
|
Three mechanisms of acquired hydrocephalus |
CSF obstruction: SOL CSF reabsorption ➘: Infection or haemorrhage CSF production ➚: choroid plexus papilloma |
|
|
Paient suffers from headache, blurred vision and drop-attacks. What is the likely diagnosis? What other sign would you look for to support the diagnosis? What is a possible complication? How will you treat it? |
Hydrocephalus
Supported by papilloedema and increased head circumference Complication: herniation Treatment: Ventriculo-peritoneal shunt Endoscopic ventriculostomy (hole for drainage) |
|
|
Most common brain tumour in adults and infants |
Infants: Medullobastoma Adults: Glioblastoma |
|
|
Treatment for gliobastoma, medulloblastoma and meningioma. Are they curable? |
Glioblastoma - Radio + Chemo (no surgery) ➙ Not curable Medulloblastoma - Surgery + Radio + Chemo ➙ Long term remission Meningioma - Surgery ➙ Curable |
|
|
Cells of origin of gliobastoma, medulloblastoma and meningioma. |
Glioblastoma - Astrocytes Medulloblastoma - Immature or embryonal cells Meningioma - Arachnoid “cap” cells of meninges (i.e. cells of the arachnoid granulations) |
|
|
Most likely site of gliobastoma, medulloblastoma and meningioma. |
Glioblastoma - Hemispheres Medulliobastoma - Vermis (cerebellum) Meningioma - Anywhere |
|
|
How do the following tumours propagate: gliobastoma, medulloblastoma and meningioma? |
Glioblastoma - Follows WM pathways Medulloblastoma - Spreads via CSF Meningioma - Usually don't propagate |
|
|
Histological presentation of gliobastoma, medulloblastoma and meningioma. |
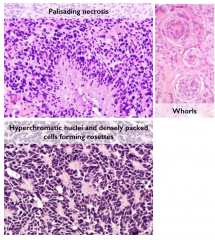
Glioblastoma Atypical, mitotically active, infiltrating astrocytes Aggregation of Aϕ around a necrotic centre (palisading necrosis) Medulloblastoma Resembles neuroblasts with hyperchromatic nuclei and little cytoplasm Cells are densely packed and may form rosettes Meningioma Lobules of meningothelial cells with concentric whorls that are called psammoma bodies when calcified |
|
|
What brain tumour typically presents as rosettes on histology |
Medulloblastoma |
|
|
What brain tumour typically presents as palisading necrosis on histology |
Glioblastoma |
|
|
What brain tumour typically shows whorls on histology |
Meningioma |
|
|
Name two tumours of the peripheral nerve sheath |
Neurofibroma Schwannoma |
|
|
How do neurofibroma and schwannoma differ (3)? |
Neurofibroma Contains Schwann cells and fibroblasts Infiltrate parent nerve/Non-encapsulated Part of Neurofibromatosis Type 1 Schwannoma Contains Schwann cells only Compresses parent nerve without infiltrating/Encapsulated Part of Neurofibromatosis Type 2 |
|
|
Pattern of inheritance of neurofibromatosis |
Autosomal dominance |
|
|
Name 3 tumours that are part of neurofibromatosis type 1 and 3 for type 2 |
Type 1 Neurofibroma Glioma (esp. optic nerve astrocytoma) Phaeochromocytoma Café au lait spots Type 2 Bilateral vestibular schwannoma Peripheral Schwannoma Meningioma |
|
|
How can brain swelling be diagnosed in vivo and postmortem? |
Flattened gyri (on MRI or brain slices) |
|
|
What type of tumour mostly metastasise to the brain and how do they metastasise? |
Carcinomas are the most common tumour type to metastasise to the brain, but lymphoma can also do so. Metastatic deposits are blood-borne |
|
|
Confirmation of malignant meningitis |
CSF cytology
|
|
|
What is butterfly glioma |
Spread of a glioblastoma through the corpus callosum |
|
|
Relation between glioma and astrocytoma and glioblastoma |
Glioma: Tumour of glial cells Astrocytoma: Tumour of the astrocytes Glioblastoma: Grade 4 astrocytoma ⇒ Gliobastoma is an astrocytoma that is a glioma |
|
|
Why can there be haemorrhage in the presence of glioblastoma of the temporal lobes? What is the outcome? |
Tumour in temporal lobe ⇒ Transtentorial herniation ⇒ Haemorrhage in the brainstem (Duret’s haemorrhage) ⇒ Death |
|
|
True or false: the grade of a brain tumour is the best factor to predict prognosis |
False, its location and size are more important |
|
|
Tumours in the cerebellopontine angle causing hearing loss. On imaging, tumour appears benign. What is it likely to be? Significance of the presence of this tumour bilaterally? |
Vestibular schwannoma Bilateral ⇒ Likely from neurofibromatosis type 2 |
|
|
Name one cause of stroke that is not due to the occlusion of an artery nor an haemorrhage. What are its aetiologies (4)? |
Venous infarction (esp. sagittal sinus thrombosis) Aetiologies: Infection, pregnancy, hypercoagulable state, trauma |
|
|
Name one artery that, if rupture, may cause extradural haemorrhage |
Middle meningeal artery (it runs between the dura and the skull) |
|
|
What type of haemorrhage does a berry aneurysm cause? |
Subarachnoid haemmorhge |
|

Diagnosis? |
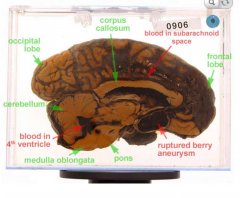
Ruptured berry aneurysms ⇒ SAH |
|
|
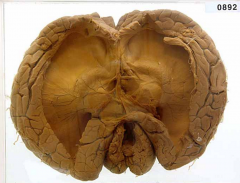
Hydrocephalus |
|
|
What is gliosis? |
The process of scar tissue formation by astrocytes (the scar is not made of fibrous tissue as elsewhere in the body but by glial tissue) |
|
What is the disease? |
MS (plaques of grey areas in the white matter, esp. around ventricles) |
|
|
LP reveals oligoclonal bands of immunoglobulin in CSF. Name a likely diagnosis? |
MS |
|
|
3 clinical hallmarks of Parkinson's disease |
Resting tremor Bradykinesia Rigidity |
|
|
Pathogenesis of Parkinson's disease |
Degeneration of dopaminergic pigmented cells of substantia nigra |
|
|
Macroscopic appearance of PD |
Pallor of substantia nigra |
|
|
Microscopic appearance of PD |
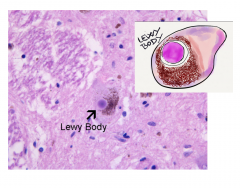
Lewy bodies: Accumulation of α-synuclein inside nerve cells |
|
|
Post-mortem histology of base of brain shows accumulation of α-synuclein inside nerve cells. Likely diagnosis? |
PD |
|
|
Two treatment of PD |
L-Dopa DBS |
|
|
Three clinical hallmarks of Huntington's disease |
Chorea Psychiatric symptoms Dementia |
|
|
Pattern of inheritance of Huntington's disease |
Autosomal dominant with anticipation |
|
|
Pathogenesis of Huntington's disease |
Toxic gain of function of mutated huntingtin gene ➙ Degeneration of cortico-striatal loops |
|
|
Macroscopic appearance of Huntington's disease |
Atrophy of head of caudate nucleus and cerebral cortex |
|
|
Microscopic appearance of Huntington's disease |
Aggregation of polyglutamine-containing fragments of huntingtin in nuclei and neurites of neurons |
|
|
Histology reveals aggregation of polyglutamine-containing fragments of huntingtin in nuclei and neurites of neurons. Diagnosis?
|
Huntington's |
|
|
Clinical presentation if Alzheimer's disease
|
Dementia (early: short term memory impairment, late: dysphasia and apraxia) |
|
|
Mutation of amyloid precursor protein is a risk factor to what neurological disease |
Alzheimer's |
|
|
Mutation of ApoE with presence of ε4 is a risk factor of what neurological disease |
Alzheimer's (positive risk factor) |
|
|
Mutation of ApoE with presence of ε2 is a risk factor of what neurological disease |
Alzheimer's (negative risk factor) |
|
|
Down’s syndrome is a risk factor for what neurological disease |
Alzheimer's |
|
|
What lobes are particularly affected in Alzheimer’s disease |
Medial temporal atrophy followed by neocortical atrophy |
|
|
What striking feature of Alzheimer's disease is visible on MRI? |
Hydrocephalus (compensatory for medial temporal atrophy and neocortical atrophy) |
|
|
Histology reveals extracellular deposition of β-A4 peptide in cortical plaques. Likely diagnosis? |
Alzheimer's |
|
|
Histology reveals extracellular deposition of β-A4 peptide in vessels. Likely diagnosis? |
Alzheimer's |
|
|
Histology reveals intracellular deposition of protein tau as neurofibrillary tangles. Likely diagnosis? |
Alzheimer's |
|
|
Treatment for Alzheimer's disease |
Cholinesterase inhibitors to soothe symptoms |
|
|
Macroscopic appearance of Alzheimer's disease
|
Medial temporal atrophy followed by neocortical atrophy and compensatory hydrocephalus |
|
|
Clinical presentation of CJD |
Very variable but classically, rapidly progressive dementia |
|
|
What neurological disease can be acquired with mad cow disease |
Bovine spongiform encephalopathy (BSE) ➙ CJD |
|
|
Genetic test in patient is positive for Polymorphism of PRNP codon 129. What is the patient at risk of? |
CJD (PRNP stands for PRioN Protein) |
|
|
Pathogenesis of CJD |
Prion protein (normal) becomes a prion (abnormal) and that prion causes other prion proteins in the body to because prion themselvesIn CJD, the prion protein is PrPC, whereas the prion is PrPSc. |
|
|
3 aetiologies of CJD |
Sporadic Inherited Acquired (e.g. mad cow) |
|
|
Microscopic appearance of CJD |
Triad: Spongiosis, neuronal loss, gliosis |
|
|
What test would you do to definitely diagnose CJD |
Check for deposition of PrPSc is diagnosis |
|
|
Deposition of PrPSc detected on histology of synapses. Diagnosis? |
CJD |
|
|
A patient has a genetic test for a research study and is found to have two copies of the Huntingtin gene (HTT), which codes for the protein Huntingtin (Htt). What should you tell him and his family? |
Nothing, this is normal. Everyone has two copies of the Huntingtin gene (HTT), which codes for the protein Huntingtin (Htt). Patients with HD have a mutated version of that gene. |
|
|
Significance of left pronator drift |
Focal pathology on the right |
|
|
Sudden onset of severe thunderclap headache is the presentation of what haemorrhage? |
Spontaneous subarachnoid haemorrhage |
|
|
Clinical presentation of intracerebral haemorrhage |
Sudden onset focal neurological deficit (stroke) ± collapse |
|
|
Three contraindications (officially, i.e. for the exam) to LP without prior CT |
New focal neurological signs Reduced level of consciousness Papilloedema (a relatively late sign of raised intracranial pressure) |
|
|
3 complications of SAH secondary to aneurysm
|
Re-bleeding of the aneurysm Hydrocephalus Vasospasm |
|
|
Patient with SAH secondary to aneurysm rupture has deteriorating GCS score. Why can it be and what is the first investigation to confirm the diagnosis? |
Any complication of SAH (re-bleeding, hydrocephalus, vasospasm) can be the cause. Rebleeding and hydrocephalus would both be detected on CT.
|
|
|
"Worst headache ever" is typically a sign of which haemorrhage? |
SAH |
|
|
Why would you monitor U&E in patients with any acute intracranial pathology? |
Risk of SIADH |
|
|
What collagen forms the bone matrix |
Type 1 |
|
|
Effect of oestrogen on bone metabolism. Consequence for menopause and hypogonadism |
Oestrogen reduce bone resorption, increase bone formation ⇒ Menopause and hypogonadism are RF for osteoporosis |
|
|
4 endocrine diseases that may cause osteoporosis |
Hyperparathyroidism Hyperthyroidism (increase metabolic rate of bone replacement) Hypogonadism (⇒ oestrogen ➘ ⇒ bone reabsorption ➚ and bone formation ➘) Cushing's (⇒ Cortisol ➚ ⇒ Calcium release from bone ➚) |
|
|
Two non-modifiable risk factors and two lifetime risk factors of osteoporosis |
Female >50 Smoking, alcohol |
|
|
Definition of osteoporosis |
Bone mineral density < µ - 2.5σ |
|
|
Define rickets and osteomalacia |
Rickets Failure to mineralise new bone at growth plates (children) Osteomalacia Failure to mineralise new bone (adults) |
|
|
Most likely aetiology of rickets and osteomalacia. What other broad aetiology exists? How are they distinguished? |
Vitamin D deficiency Phosphate deficiency (e.g. Fanconi's syndrome, X-linked hypophosphataemic rickets) In phosphate deficiency, Vit D ➚ |
|
|
3 S&S of rickets and osteomalacia |
Bone pain Muscle weakness Multiple bone deformities Fractures Short stature |
|
|
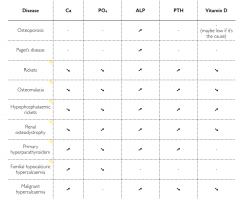
How are CaPO4ALPPTHVitamin D in: Osteoporosis Piget's Ricket's Osteomalacia Hypophophataemic rckets Renal osteodystrophy Primary hyperparathyroidism Familial hypocalciuric hypercalcaemia Malignant hypercalcaemia |
|
|
|
What is Fanconi’s syndrome? |
Disease of the PCT in which glucose, AA, uric acid, PO4 and HCO3 are passed into the urine, instead of being reabsorbed. |
|
|
How are Paget's disease and osteoporosis differentiated? |
Paget's: Bone deformity Osteoporosis: Bone hypodensity |
|
|
Common sites of Paget's |
Pelvis Vertebrae Skull Tibia |
|
|
Deafness with raised ALP is a flag for what disease? |
Paget's |
|
|
You suspect Paget's in one of your pt based on symptoms and raised ALP. What is the first line of investigation? |
Plain XR |
|
|
Pathogenesis of renal osteodystophy |
Chronic renal disease ⇒ Excretion of PO4 ➘ and Vitamin D is not activated ⇒ Hyperphosphataemia and Hypocalcaemia ⇒ Hyperparathyroidism ⇒ Bone reabsorption by osteoclasts ⇒ Osteodystrophy |
|
|
One complication of treatment of renal osteodystophy |
Adynamic bone disease: Vit D ➚ ⇒ PTH suppression ⇒ Chronic suppression of bone turnover |