Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
45 Cards in this Set
- Front
- Back
|
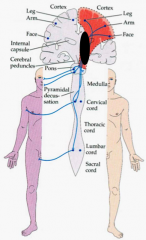
What is the least number of neurons it takes to transmit an impulse from motor cortex to muscle fiber? Which are |

Two - UMN traveling via LCST and an LMN (α motor neuron) that exits spinal cord
|
|
|
What controls contralateral muscle movement?
|
Lateral Corticospinal Tract
|
|
|
Where can you localize a muscle weakness to?
|
- Lesion in cortex
- Lesion in brainstem - Lesion in spinal cord |
|
|
What are some signs of a lesion to the lateral corticospinal tract in the cortex?
|
- Contralateral weakness and aphasia (inability to understand or express language)
- Apraxia (inability to do a learned movement, e.g., brushing teeth) - Neglect (ignore stimuli on one side of body) |
|
|
What are some signs of a lesion to the lateral corticospinal tract in the brainstem?
|
Ipsilateral CN findings and contralateral body weakness
|
|
|
What are some signs of a lesion to the lateral corticospinal tract in the spinal cord?
|
Weakness below a certain spinal cord level
|
|
|
What is a Hemicord lesion? Name?
|
- Weakness on one side and sensory loss on other
- Begins at a certain spinal cord level and below - AKA: Brown-Sequard Syndrome |
|
|
What is the function of the Corticobulbar Tract?
|
Controls contralateral facial movement
|
|
|
If you lesion the UMN of the corticobulbar tract, what are the symptoms?
|
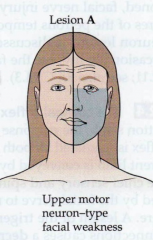
- Contralateral weakness of lower face (mouth droop; flat nasolabial fold)
- Intact forehead wrinkle |
|
|
If you lesion the LMN of the corticobulbar tract, what are the symptoms?
|
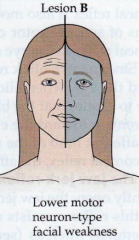
- CN VII lesion
- Ipsilateral upper and lower facial weakness - Bell's Palsy |
|
|
What is the function of the Reticulospinal tracts?
|
- Unconscious motor control
- Give muscles "tone" - Inhibits the LMN, which is tonically active |
|
|
Which muscles/LMNs have more tone?
|
- Antigravity muscles/LMNs - muscles that help you walk/move against gravity
- E.g., quadriceps, tibialis anterior, biceps, etc. - Arms - flexors - Legs - extensors |
|
|
If you increase activity of the UMN, what happens to the LMN and muscle?
|
- Inhibit LMN
- Muscle relaxes |
|
|
If you decrease activity of the UMN, what happens to the LMN and muscle?
|
- Lose inhibition of LMN
- Muscle contracts |
|
|
What happens if there is a lesion to the Reticulospinal Tract?
|
- Acute lesion (e.g., acute stroke) - contralateral hypotonia (system is in shock so no tone)
- Chronic lesion (e.g., chronic stroke) - contralateral hypertonia (because decreased inhibition of LMN) |
|
|
What causes hyperreflexia?
|
UMN to the α-MN is lesioned
|
|
|
What causes hyporeflexia?
|
LMN is lesioned; or lesion of afferent or efferent limb
|
|
|
What are the deep tendon reflexes?
|
- Biceps
- Brachioradialis - Triceps - Pateller - Achilles |
|
|
What nerve is involved in the biceps reflex? At what level?
|
- Musculocutaneous N.
- C5 |
|
|
What nerve is involved in the brachioradialis reflex? At what level?
|
- Radial n.
- C6 |
|
|
What nerve is involved in the triceps reflex? At what level?
|
- Radial n.
- C7 |
|
|
What nerve is involved in the Patellar reflex? At what level?
|
- Femoral n.
- L2/3 |
|
|
What nerve is involved in the Achilles reflex? At what level?
|
- Sciatic n.
- S1 |
|
|
How does an UMN lesion affect:
- Tone - Reflexes - Atrophy - Fasciculations - Weakness |
- Spasticity (high tone)
- Hyperreflexia - No/mild atrophy - No fasciculations - Spastic paresis (weak, slow movement) |
|
|
How does an LMN lesion affect:
- Tone - Reflexes - Atrophy - Fasciculations - Weakness |
- Decreased tone
- Hyporeflexia - Significant atrophy - Fasciculations - Flaccid paresis |
|
|
What are the symptoms of an anterior horn cell lesion?
|
* LMN lesion: aka α-MN
- Flaccid paralysis - Severe atrophy - Fasciculations - spontaneous firing of motor neuron (twitching under skin, not painful) - Cramping - firing of multiple motor neurons or entire muscle, entire muscle contracts (painful) - Loss of reflexes |
|
|
What are some examples of Anterior Horn Cell Lesion?
|
ALS, polio
|
|
|
What are the symptoms of a root lesion?
|
- Shooting pain in a root dermatomal distribution
- Loss of reflexes that correspond to root - Little or no weakness and atrophy (would need to have all roots lesioned) |
|
|
What can cause a root lesion?
|
Disc herniation
|
|
|
What are the symptoms of a plexus lesion?
|
- Multiple muscles in arm or leg involved
- Loss of reflexes (depends on localization) - Sensory loss depending on localization - Usually painful |
|
|
What are some examples of Plexus lesions? What do they affect?
|
- Erb's Palsy - upper trunk of brachial plexus
- Klumpke's Palsy - lower trunk of brachial plexus - Pancoast tumor - lower trunk of brachial plexus - Diabetic lumbosacral plexopathy - lumbosacral plexus |
|
|
What are the characteristics of Erb's Palsy?
|

- Arm held internally rotated, extended at elbow, flexed at side of body
- "Waiter's tip" pose - Can fully move hand - Can be caused in birthing process when neck is stretched * Due to upper trunk of brachial plexus lesion * |
|
|
What are the characteristics of Klumpke's Palsy?
|

- Opposite of Erb's
- Weakness in fingers, but no difficulty moving across shoulder and elbow - Can be caused when hanging from tree * Lesion of lower trunk of brachial plexus * |
|
|
What are the symptoms of a Pancoast tumor?
|
- Tumor of apical part of lung (if your patient is a smoker and losing weight with these symptoms, worry about this)
- Lower trunk of brachial plexus lesion - Similar symptoms as Klumke's (weakness in fingers but not across shoulder or elbow) |
|
|
What happens in a peripheral nerve lesion?
|
- Muscles innervated by that nerve show profound atrophy
- Dense sensory loss - Reflexes may be lost if muscle tested is innervated by lesioned nerve |
|
|
What is an example of a peripheral nerve lesion?
|
Carpal Tunnel Syndrome
|
|
|
What is compressed in Carpal Tunnel Syndrome? Cause?
|

- Median nerve compression at wrist (neuropathy)
- Caused by overuse of finger flexors from repetitive tasks cause these muscles to hypertrophy - Hypertrophied muscles and median nerve pass through tunnel, which is a confined space - Muscles compress nerve as they grow |
|

What are the symptoms of Carpal Tunnel Syndrome?
|

- Pain and tingling in median region of hand (thumb to lateral half of ring finger) - symptoms in thumb to middle finger common
- Especially bothersome at night because hand gets accidentally hyperflexed at wrist and patient wakes up and shakes out hand - If chronic, can cause atrophy of median innervated hand muscles causing loss of bulk and thenar eminence |
|
|
What happens in a NMJ defect?
|
- Fatigable weakness (worse later in day and after repetitive movements, improved after rest)
- Affects muscles that are constantly working (levator palpebrae, extraocular muscles, neck extensors, core muscles, swallowing muscles, intercostals/diaphragm) |
|
|
Symptoms of NMJ defect?
|
- Occur later in the day and after repetitive movement
- Ptosis - Diplopia (double vision) - Dropped head - Difficulty rising from chair, stairs - Dysphagia (difficulty swallowing) - Difficulty breathing (intercostals/diaphragm) - No sensory loss - Reflexes normal - No muscle atrophy |
|
|
What are some causes of NMJ defects?
|
- Myasthenia
- Lambert-Eaton myasthenic syndrome - Botulism |
|
|
What are the symptoms of a muscle lesion?
|
- Weakness in certain muscle groups
- Normal sensation - Intact reflexes (unless there is profound muscle atrophy) |
|
|
What are some examples of muscle lesions?
|
- Myositis (inflammation and degeneration)
- Muscular dystrophies (Duchenne's) - defect in enzymatic function or structural defects |
|
|
Case: 31 yo F developed sudden R f/a/l weakness 2 weeks ago
- Mild slurred speech - Falling - No sensory loss, headache - Exam: Vitals: normal - Normal language; no neglect - ↓R nasolabial fold - ↑tone in R arm; R finger taps slow - 4+/5 strength in R arm/leg - Reflexes 3+ on R arm/leg - Spastic gait Localize?? |
* L posterior limb of internal capsule
- L LCST/corticobulbar at internal capsule or L pons - Stroke or MS - No cortical signs & leg involved (so has to be 2 vascular territories) - No spinal level --> not cord - R pure motor problem with UMN signs --> LCST on L lesioned - R UMN facial weakness --> L corticobulbar tract (before pons) |
|
|
- Case: 62 yo F with DM, HTN develops sudden aphasia and R face/arm weakness
- Exam: Speech is halting, effortful, agrammatic, few words - L gaze preference - R lower facial weakness - R arm drift; leg normal - R arm/face sensory deficit - Ref lexes: absent in RUE; normal elsewhere; Babinski absent on L and mute on R Localize (neural axis & vascular distribution)?? |
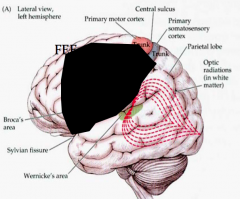
L frontal cortex and parietal cortex
(MCA distribution) - Stroke - Broca’s aphasia --> L frontal cortexcortical sign - L gaze preference --> R FEF working --> L FEF lesioned --> cortical sign - R lower face & arm --> L frontal cortex - R arm/face sensory deficit --> L parietal cortex - Reflexes ↓ b/c acute |