Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
46 Cards in this Set
- Front
- Back
|
What is the purpose of eye movements? |
- Maintain visual input on center of macula, FOVEA, where visual acuity is highest due to high density of cones
- Ability to fixate |
|
|
What kind of movements are needed to fixate on an object?
|
- Horizontally / Vertically
- Converge / Diverge - Conjugate eye movements - yoked together |
|
|
Which pathway mainly keeps the eyes together?
|
Medial Longitudinal Fasciculus (MLF)
|
|
|
What are the two systems for eye movements?
|
- Fast, voluntary system - Saccadic system
- Slow, involuntary system |
|
|
What are the components of the Fast Eye Movement system? Functions?
|
Saccades - voluntarily brings objects in peripheral vision onto fovea (under cortical control)
|
|
|
What are the components of the Slow Eye Movement system? Functions?
|
- Smooth pursuit system - voluntarily follow a moving object (cortex)
- Vestibulo-ocular reflex (VOR) - involuntarily coordinate eye and head movement to stabilize object on fovea (vestibular system) - Optokinetic system - involuntarily stabilizes object on fovea during sustained head rotations |
|
|
How do the fast and slow eye movement systems come together to move the ey?
|
Final common pathway - cranial nerve nuclei involved in extraocular movement
|
|
|
What are two main symptoms related to eye control?
|
- Diplopia
- Nystagmus |
|
|
What is Diplopia?
|
Double vision - neurological issue (unlike blurred vision)
|
|
|
What causes diplopia?
|
Image not resting on the fovea of each eye due to muscle, NMJ, nerve, or CNS disorder
|
|
|
What is blurred vision? Cause?
|
- Decreased visual acuity
- Neurological or non-neurological cause - E.g., corneal abrasion, optic neuritis, etc. |
|
|
What is Nystagmus?
|
Fast oscillatory eye movements (more than 1-2 beats)
|
|
|
What causes nystagmus?
|
- Defect of slow eye movement system (usually impaired VOR)
- Need to have intact cortex (frontal eye fields) to get nystagmus |
|
|
What are the phases of the Nystagmus?
|
- Fast phase - mediated by cortex
- Slow phase - VOR not working (R nystagmus = L VOR not working) |
|
|
If the patients eyes are beating vertically (vertical nystagmus), what is the cause?
|
ALWAYS a CNS lesion
|
|
|
If the patients eyes are beating horizontally or rotationally (horizontal or rotational nystagmus), what is the cause?
|
CNS or PNS lesion
|
|
|
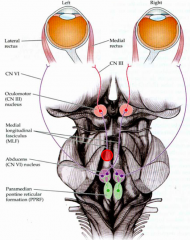
What nucleus helps eyes move horizontally?
|
Abducens Nucleus/PPRF = Horizontal Gaze Center
|
|
|
How do you get your eyes to simultaneously look L?
|
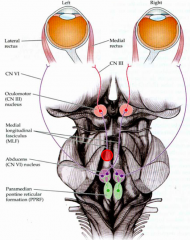
L abducens nucleus / PPRF --> moves both eyes to L:
- L CN VI pulls L lateral rectus to move eye L - Sends signal to R CN III to pull R medial rectus to move eye L |
|
|
What is the function of the Medial Longitudinal Fasciculus (MLF)?
|
- Yolks eyes together
- Helps contralateral eye adduct (look medially) |
|
|
What is the term for a lesion to the Medial Longitudinal Fasciculus (MLF) of one side? What happens?
|
- Internuclear Ophthalmoplegia (INO)
- R MLF lesion causes R INO, R eye does not adduct and L eye has nystagmus on leftward gaze - L eye nystagmus because of double vision (due to R eye not adducting) |
|
|
When there is a lesion to the MLF (causing internuclear ophthalmoplegia, INO), what causes the other eye to have a nystagmus?
|
- Double vision due to other eye not adducting)
- VOR moves eye back towards nose, but because of instructions to look away from nose, the cortex overrides (suppresses VOR) and moves it back where you want it to look - Looks like the eye with nystagmus is trying to "pull" the other eye over |
|

What's wrong in this patient?
(Only one eye moves towards right) |
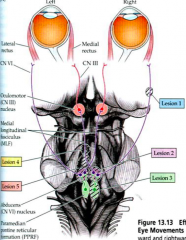
- Lesion to right abducens nerve (CN VI palsy)
- R lateral rectus is not moving eye adequately, innervated by R CN VI) (Lesion 1) |
|

What's wrong in this patient?
(Neither eye moves towards right) |
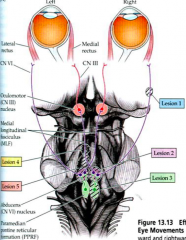
- Lesion (2) to right abducens nucleus (R lateral gaze palsy)
OR - Lesion (3) to right PPRF (R lateral gaze palsy) |
|

What's wrong in this patient?
|
- Lesion (4) to L MLF (L INO)
- L eye won't move to right (no input to L medial rectus) - R eye exhibits nystagmus due to double vision and opposing inputs from VOR/cortex |
|

What's wrong in this patient?
|
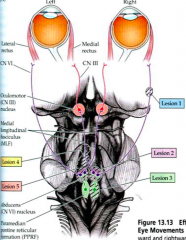
- Lesion (5) to L MLF and L abducens nucleus (1-1/2 syndrome)
- Can't look left with either eye because of lesion to L abducens nucleus - Can't look right with L eye because of lesion to L MLF - R eye looking R has nystagmus due to opposing inputs from VOR / cortex |
|
|
What is the function of saccades? What mediates it?
|
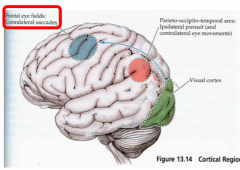
- Move eyes to object of interest (foveation) very quickly (>700 degrees/sec)
- Voluntary - mediated by cortex: contralateral Frontal Eye Fields (FEF) * If you want to look quickly at something on your R, use L FEF |
|
|
What is the pathway to make you look to the R very quickly?
|
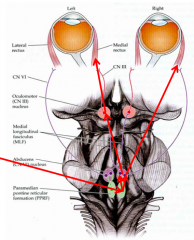
- Activate L frontal eye fields (FEF)
- Activates R PPRF / Abducens Nucleus - R CN VI - lateral rectus turns R eye to right - L MLF activates L oculomotor nucleus & L CN III - medial rectus turns L eye to right - Both eyes move right |
|
|
What are the two types of clinical consequences of lesions to the saccadic system?
|
- Right-way eyes
- Wrong-way eyes |
|
|
What are the symptoms of Right-Way Eyes? Cause?
|

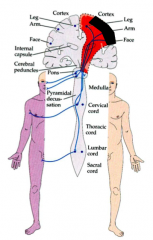
- Contralateral hemiparesis
- Ipsilateral gaze preference - Frontal Cortex lesion (lesion to side eyes are looking) |
|

Why is there contralateral hemiparesis and ipsilateral gaze preference in "right-way eyes"?
|

- Contralateral hemiparesis - lesion of primary motor cortex
- Ipsilateral gaze preference - frontal eye field lesion does not allow saccading to opposite side, but opposite side FEF is still functional and causes eyes to look toward lesion |
|

What can cause "Right-Way Eyes"?
|
Frontal cortex stroke (on side that the eyes are looking towards, opposite side of hemiparesis)
|
|
|
What are the symptoms of "Wrong-Way Eyes"? Cause?
|

- Contralateral hemiparesis
- Contralateral gaze preference - Lesion to pons |
|

Why is there contralateral hemiparesis and contralateral gaze preference in "wrong-way eyes"?
|

- Contralateral hemiparesis - L pontine corticobulbar / corticospinal tracts --> causes R body/face paresis
- Contralateral gaze preference - L PPRF/abducens nuclei lesion --> loss of L horizontal gaze center --> cannot look to left (so eyes deviate to R / contralateral side) |
|
|
What allows you to track a moving object smoothly?
|
- Smooth pursuits
- If object is moving faster than ability of smooth pursuit system to follow, then saccadic system takes over |
|
|
What mediates the Smooth Pursuits system?
|
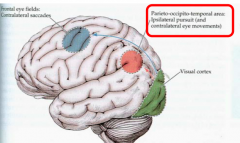
- Parieto-Occipital-Temporal eye fields
- Stimulate ipsilateral PPRF/abducens nucleus - Modulated by cerebellum (flocculonodulus) |
|
|
What happens if there is a lesion to smooth pursuit system?
|
"Jerky" eye movements because saccades are being used instead
|
|
|
What can cause "jerky" eye movements?
|
- Lesion to smooth pursuits system (instead using saccades)
- R parietal-occipital-temporal lesion (jerkiness to R) - Lesion of cerebellum can also cause jerky pursuits - R parietal eye field lesion --> inability to pursue to R |
|
|
What mediates the Vestibulo-ocular reflex (VOR)?
|
- Vestibular nuclei / nerve and semicircular canals (SCC)
- Influenced/inhibited by cerebellum (flocculonodular lobe) |
|
|
Which way does the VOR move your eyes?
|
Contralaterally: if head moving to left, eyes move to right
- Specifically, turn head left, activating L ear horizontal SCC --> moves eyes to right |
|
|
What are the symptoms if the VOR is lesioned?
|
- Every time you move head, images can't be stabilized on fovea
- Everything in field of vision will blur and result in lowered visual acuity (feeling dizzy too) |
|
|
What can cause the VOR to not work correctly?
|
- Gentamycin toxicity
- Bilateral vestibular dysfunction |
|
|
How do you suppress the VOR?
|
Cortex (such as FEF - frontal eye fields)
|
|

What is wrong with this patient?
|

- R CN VI lesion OR R Lateral Rectus lesion
- R eye is esotropic (inward) on primary gaze - R eye does not fully abduct |
|

What is wrong with this patient?
|
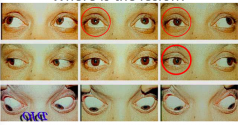
Impaired R eye adduction --> R Internuclear Ophthalmoplegia --> R Medial Longitudinal Fasciculus (MLF) lesioned
|
|

What is wrong with this patient?
|

- Cannot look L --> L horizontal gaze center lesion --> L abducens nucleus / PPRF
- Cannot look R --> R horizontal gaze center - Intact up, down, convergence --> intact CN III and IV * Bilateral Abducens nucleus / PPRF lesions |
|

What is wrong with this patient?
|

- Impaired R eye adduction --> R INO --> R MLF
- Impaired R gaze --> R horizontal gaze center --> R abducens nucleus (and/or PPRF) * 1-1/2 syndrome * |