![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
163 Cards in this Set
- Front
- Back
|
typical subtests of the ENG/VNG Battery |
|
|
|
components of oculomotor and gaze stabilization |
|
|
|
components of positional and positioning |
|
|
|
components of caloric testing |
response and fixation |
|
|
advantages of ENG/VNG (over other vestibular tests) |
|
|
|
limitations of ENG/VNG (over other vestibular tests) |
|
|
|
a normal ENG?VNG CANNOT indicate completely normal vestibular function |
know know |
|
|
oculography |
recording of eye movement |
|
|
nystagmography |
recording or nystagmus |
|
|
How can recordings be obtained? |
electrical infrared video other |
|
|
What do you look for in examination of eye movements |
horizontal vertical torsional (rotary) nystagmus (strength and suppressibility) |
|
|
symptom impression and elicitation |
|
|
|
What does failure to recognize disconjugate eye movements result in? |
faulty measurement of eye movements because averaged signals do not accurately reflect actual movements of either eye |
|
|
for disconjugate eye movements change the standard protocol to record either... |
|
|
|
what does oculomotor testing document? |
abnormalities of the oculomotor system that can confound interpretation of vestibular test results |
|
|
What anatomical system does oculomotor testing provide a "look" at? |
the several critical CNS system areas |
|
|
How can you examine eye movement? |
|
|
|
electric oculography |
|
|
|
When looking right, the potential increases in the electrode beside the (right/left) eye and decreases the (right/left) during electric oculography |
right, left |
|
|
For horizontal recording, where are electrodes placed during electric oculography? |
at the corner of the eye |
|
|
For vertical recording, the electrodes are placed where during electric oculography? |
above and below the eyes |
|
|
deficiencies of horizontal and vertical recording |
|
|
|
preparing the electrode site during electric oculography |
impedance is not as important as long as impedance is roughly equal |
|
|
two channel system works for most recordings providing (electric oculography) |
|
|
|
eye motion analysis during infrared oculography |
|
|
|
how is the eye illuminated on the infrared light? |
|
|
|
deficiencies of infrared oculography |
|
|
|
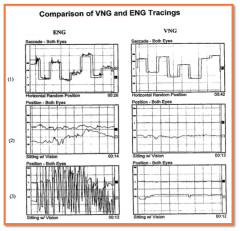
ENG and VNG recordings |
|
|
principle measures during oculomotor and gaze testing |
|
|
|
the most important part of the operator is to be... |
|
|
|
procedures for calibrations |
|
|
|
When is repeated calibration essential? |
for ENG due to changes in the electrode/skin interface over time or slight shifts in the camera system relative to the eyes |
|
|
Where does oculomotor tests evaluate eye movements originating from... |
the cerebellum |
|
|
abnormalities during oculomotor tests |
may indicate neurologic disease |
|
|
referrals for oculomotor tests should be based on... |
patient history and abnormal results |
|
|
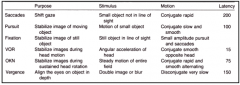
procedure for saccade testing |
|
|
|
What do you ask the patient to avoid during saccade testing? |
head movement and not to anticipate target movements |
|
|
saccade testing clinically measures... |
|
|
|
What are results of saccade testing compared to? |
age wighted norms |
|
|
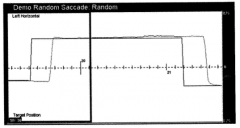
normal saccade |
|
|
What is the goal of saccade eye movements? |
to fixate accurately and quickly on a new target (eye movements should be equal in amplitude and distance from one target to the next) |
|
|
abnormalities of saccade testing |
|
|
|
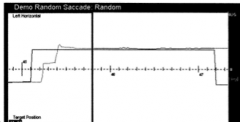
undershoots |
|
|
|
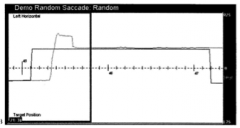
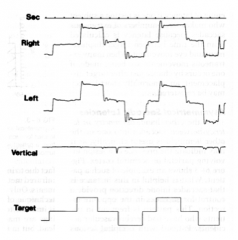
overshoots |
|
|
|
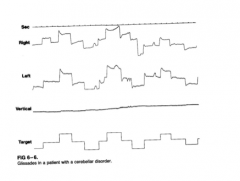
glissades |
saccade "glides" to an end point; eye drifts toward or away from the target |
|
|
pulsion |
vertical saccades are "pulled" to the left or right |
|
|
saccade undershoot - hypometria |
|
|
saccade overshoot - hypermetria |
|
|
saccade glissade |
|
|
saccade overshoot |
|
|
how is saccade velocity measured? |
as the peak speed of eye movement when moving from one target to another |
|
|
abnormal saccade velocity |
consistency slower than 430 degrees per second for large amplitude saccades
consistent lower than 200 degrees per second for small amplitude saccades |
|
|
saccade latency |
difference in time from then target is presented and eyes start to move |
|
|
latency for random target |
150-25 msec |
|
|
latency for predictable target |
76 msec |
|
|
abnormal saccade latency |
a consistent delay of 260 or longer |
|
|
saccade morphological abnormalities |
slowing internuclear ophthalomoplegia (MLF lesion) |
|
|
slowing morphological abnormality |
saccadic central pathways, pontine gaze centers, defects in OM system (neural centers and ON muscles), MLF lesions, myasthenia gravis, hunting tons disease |
|
|
internuclear ophthalmoplegia |
|
|
|
pitfalls of saccade interpretation |
|
|
|
what do you ask the patient to do during smooth pursuit? |
to follow a target that moves smoothly back and forth (like a pendulum) |
|
|
what is the goal of smooth pursuit? |
to maintain gaze on a moving target |
|
|
principle clinical measures during smooth pursuit |
|
|
|
smooth pursuit is produced and controlled where in the CNS? |
|
|
|
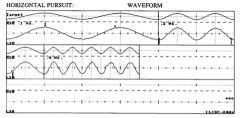
smooth pursuit |
|
|
difficulties in using smooth pursuit to specify clinical abnormalities |
due to verity of factors, the diagnostic specificity supplied by pursuit findings in minimal
generally utility is to establish the presence of some CNS/oculomotor system pathology
poorly defined norms due to a high level of interdependent in the test variables of frequency, amplitude, and velocianty |
|
|
abnormalities of smooth pursuit |
disorders and factors leading to smooth pursuit abnormality include (advanced age, brainstem disorders, cerebellar disorders, cerebral cortical disturbances, drug ingestion, inattention, visual disorders)
asymmetrical pursuit (parietal lobe, frontal lobe, latent nystagmus) |
|
|
smooth pursuit abnormalities |
|
|
asymmetrical pursuit |
spontaneous nystagmus gaze nystagmus |
|
|
disorganized pursuit |
poor peripheral vision due to retinal degeneration
tracking is okay periodically |
|
|
pitfalls of pursuit interpretation |
|
|
|
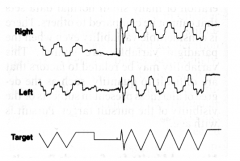
optokinetic testing |
|
|
|
clinical measures of optokinetic testing |
gain symmetry morphology |
|
|
vertical stripes can be used when testing in enclosed area such as the rotational chair (more provoking) |
know know |
|

|
optokinetic results |
|
|
When in everyday activities does the optokinetic system start when the vestibular system fails to "keep up"? |
|
|
|
What the the greatest practical utility for optokinetic testing? |
as a mechanisms to define the oculomotor system capacity to neurally and mechanically drive the eye through nystagmus as a prelude to VOR testing |
|
|
classes of eye movements and associated features |
|
|
|
gaze testing |
the patient is asked to maintain focus on a target moved and held left, right, up, down |
|
|
What is "gaze-evoked" nystagmus evidence of? |
potential CNS/oculomotor function pathology |
|
|
etiologies of gaze-evoked nystagmus |
brainstem or cerebellar disorder, ocular muscle fatigue, congenital nystagmus, normal variant, medication (nystagmus of peripheral vestibular origin is generally suppressed by gaze fixation) |
|
|
specific clinical entities of gaze testing include |
bruns nystagmus rebound nystagmus congenital nystagmus |
|
|
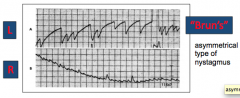
bruns nystagmus |
cerebellar lesion
asymmetrical; exponential, decreasing velocity in one direction |
|
|
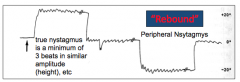
rebound nystagmus |
brainstem or cerebellar disease
occurs with transition, fades with the time in position |
|
|
congenital nystagmus |
noted at birth or shortly thereafter |
|
|
rebound nystagmus |
|
|
bruns nystagmus |
|
|
spontaneous nystagmus test |
patient is in a sitting position |
|
|
what is spontaneous gaze nystagmus testing |
for the presence of spontaneous nystagmus with and without fixation and in extremes of horizontal and vertical gaze |
|
|
degrees of gaze elicit nystagmus |
1st degree (if only in gaze direction towards fast phase)
2nd degree (if in fast phase direction and central position)
3rd degree (if in all gaze positions) |
|
|
congenital signs |
congenital nystagmus latent nystagmus |
|
|
central signs |
gaze rebound nystagmus upbeat nystagmus down beating nystagmus saccadic nystagmus internuclear ophthalmoplegia see saw nystagmus |
|
|
vestibular signs |
nystagmus in pts w/ vestibular neuritis nystagmus in pts with meniere's disease nystagmus after gentamicin treatment superior canal dehiscence - tullio |
|
|
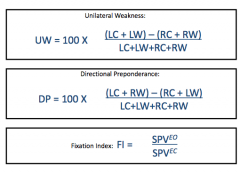
fixation in the presence of measurable nystagmus and measured in |
SP (no target) / SP (target) |
|
|
What does inability to alter fixation index strings imply? |
central involvement |
|
|
fixation |
poor suppression of nystagmus in presence of fixation |
|
|
What may result from increased fixation index? |
artifactual sources affecting pursuit such as decreased visual acuity of the effects of sedating medications |
|
|
Why must spontaneous and gaze testing be performed BEFORE positional or caloric testing? |
it can produce false positive results |
|
|
What is the rule of thumb for tasking? |
if the patient has eyes closed or VNG "windows" closed, then task |
|
|
examples of tasking exercises |
count out loud by 2's, 5's, 10's
adding, subtracting
naming categories "things you find at the beach, places you have been on vacation, your favorite books/TV shows..." |
|
|
Which tests is tasking especially important? |
position and caloric tests |
|
|
What happens when there is a failure to maintain a steady level of alertness? |
results in the nystagmus appearing and disappearing intermittently (depending on patient alertness)
nystagmus may be missed completely |
|
|
signs of central vestibular problem (pontomedullary brain stem vestibulocerebellum) when head motion or changes in head position are relative to gravity |
|
|
|
abnormal positional findings with vestibular head motion intolerance (oscillopsia and unsteadiness of gait) |
|
|
|
abnormal positional findings of the vestibular nerve |
neurovascular compression ("disabling positional vertigo") |
|
|
abnormal positional findings of the peripheral labyrinth |
|
|
|
positions for the positional test |
|
|
|
What are you determining for positional tests |
whether the vestibular system responds normally and symmetrically to position changes |
|
|
How does the system compensate following a vestibular lesion |
quickly in upright position (most frequent) |
|
|
nystagmus is not considered abnormal UNLESS |
|
|
|
types of positional findings (2) |
type I: persistent and direction changing
type II: persistent and direction fixed |
|
|
possibilities for abnormal findings (type I and II) - non-localizing |
|
|
|
directions for Dix-Hallpike |
patient is positioned on table so as to permit rapid laying down into a final position that results in the head and neck slightly extended downward
head it turned 45 degrees towards the suspected side (ipsilateral posterior semicircular canal)
patient is rapidly and smoothly moved into position |
|
|
positive finding if nystagmus (rotatory) is observed during Dix-Hallpike |
latency of 5-20 seconds
response rapidly fatigues within one minute of onset
may observe nystagmus in the reverse direction after sitting up |
|
|
What generates a response? (movement into position or final position) |
movement into position |
|
|
How can nystagmus be VISUALLY observed for Dix-Hallpike |
ENG recordings will miss rotational nystagmus (only has a vertical and horizontal recording)
VNG allows for a recording of the response - so you can document the response and go back and view it if necessary |
|
|
rotatary nystagmus towards the ground |
geotropic |
|
|
rotatary nystagmus towards the sky |
ageotropic |
|
|
What is a patient is consistent with BPPV but Hallpikes were negative? |
possible "spontaneous remission"
have the patient return is symptoms persist or return and then recheck the Hallpike |
|
|
non-classic hallpike findings |
|
|
|
anterior canal BPPV (~4% of cases of BPPV) |
evoked by Hallpike on opposite side |
|
|
How can you tell between anterior and more common posterior canal involvement? |
for posterior canal: nystagmus is geotropic (beating toward earth)
for anterior canal: nystagmus is ageotropic (beating away from earth) |
|
|
How would you treat anterior canal involvement? |
do Eply or Semont on the opposite side of the evoked response |
|
|
horizontal canal BPPV (~6% of cases of BPPV) |
may be provoked by Hallpikes on either side
symptoms are more intense with affected ear down |
|
|
positive finding for horizontal canal BPPV |
have patient lie flat and move head from left to right, if geotropic nystagmus occurs with vertigo, then its positive |
|
|
How can you treat horizontal canal BPPV? |
with a "log roll" procedure
patient lies down and rolls 360 degrees in the direction away from the affected ear |
|
|
What does caloric testing measure? |
unilateral VOR |
|
|
types of calorics |
|
|
|
What does a temperature change in the ear create? |
changes the density of the endolymph |
|
|
mechanisms for changing density of endolymph |
|
|
|
What should be done prior to caloric testing? |
otoscopy tympanometry |
|
|
why should you do otoscopy prior to caloric testing? |
look for TM perf (may confound results)
look for cerumen impaction (removal is necessary before testing) |
|
|
What should you discuss with the patient about what they will experience? |
|
|
|
How can you reduce the chances of the patient becoming sick? |
interrupt the irrigation if nystagmus intensity exceeds a critical limit
use the same time period for other irrigations |
|
|
how is patient placed for caloric testing |
patient is placed supine with head tiled 30 degrees off horizontal (horizontal SSC is situated in the vertical plane) |
|
|
when the external canal is exposed to temperature stimuli |
|
|
|
methods for irrigation |
|
|
|
advantages of air method |
|
|
|
disadvantages of air method |
|
|
|
advantages of open loop method |
|
|
|
disadvantages of open loop method |
|
|
|
advantages of closed loop method |
most effect if patient has a TM perforation |
|
|
disadvantages of closed loop method |
|
|
|
comparisons for caloric testing |
|
|
|
What happens if inadequate tasking occurs during the strongest part of the caloric response? |
the peak nystagmus velocity for that irrigation will be miscalculated |
|
|
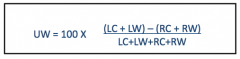
caloric test equations |
|
|
bilateral weakness caloric response |
responses from both right and left ear (total RE <12 degrees/sec and total LE <12 degrees/sec) |
|
|
directional preponderance caloric responses |
>30% alternative values 25% - 50% |
|
|
unilateral weakness |
>25% alternative values 25% - 50% |
|
|
fixation index caloric response |
>60% alternative values 50% - 60% |
|
|
hyperactive - total RE >140 degrees/sec or total LE >140 degrees/sec |
..... |
|
|
caloric test for unilateral weakness equation |
peripheral vestibular findings: WNL <28% |
|
|
caloric test for fixation suppression equation |

central finding: WNL <50% |
|
|
example of tasking for caloric testing |
give me a word in ___ category that begins with the following letter (present letters either alphabetically or randomly depending on patient) |
|
|
clinical factors for caloric irrigation |
|
|
|
order of irrigations |
start with one temperature and irrigate ears int he same order for each temperature |
|
|
wait period between irrigations |
3-5 minutes after the previous caloric nystagmus ends before starting the next irrigation |
|
|
headshake nystagmus |
a dynamic test though to be a result of asymmetry of VOR |
|
|
procedure for headshake test |
patient is asked to tilt head down 30 degrees and shake back and forth as quickly as possible for 30 seconds
patient then opens eyes and any nystagmus is observed and recorded for proper documentation |
|
|
headshake test in patients with vestibular asymmetry |
intact labyrinth generating a stronger response than the lesion side
this increased activity is stored in the velocity storage mechanism
when patient stood head shaking nystagmus is the result |
|
|
head impulse test use |
used to define inadequacy of unilateral or bilateral vestibular function |
|
|
head impulse procedure |
the patients head is rapidly turned with eyes focused on a distant object
eyes will stay on object if VOR is intact |
|
|
head impulse is VOR is insufficient to maintain position against head turn |
corrective saccade |