Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
133 Cards in this Set
- Front
- Back
|
Know that
|
|
|
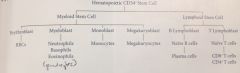
What CD#+ are Hematopoietic Stem cells?
|
CD34+
|
|
|
What is normal WBC count?
|
5-10K
|
|
|
Leukopenia
|
Low WBC count (<5K)
|
|
|
Leukocytosis
|
A high WBC count (>10K)
|
|
|
Leukopenia and/or Leukocytosis usually happens due to one cell lineage (eg. RBC, T-cell, or netrophils) being too high or too low.
TRUE OR FALSE? |
TRUE.
Know that. |
|
|
Neutropenia
What is it? |
Decreased number of circulating neutrophils
(a form of leukopenia) |
|
|
Neutropenia:
Common causes? |
Drug toxicity (some chemo agents damage stem cells resulting in decreased WBC especially neutrophils)
Severe infection (the neutrophil goes to tissues, thus decreased in circulation) (eg. severe gram negative sepsis) |
|
|
Neutropenia
Treatment? |
GM-CSF (granulocyte-macrophage colony stimulating hormone)
G-CSF |
|
|
Lymphopenia
What is it? |
Decreased number of circulating lympocytes
(a form of Leukopenia) |
|
|
Lymphopenia
Common causes? |
Immunodeficient (eg. HIV, Digeorge)
High cortisol state (induce apoptosis of lympocytes) Autoimmune destruction (SLE) Whole body radiation |
|
|
What cell is most sensitive to radiation?
|
Lymphocytes
|
|
|
Neutrophilic leukocytosis
What is it? |
Increased circulating neutrophils
|
|
|
Neutophilic leukocytosis
Common causes? |
Bacterial infection/tissue necrosis - due to increased inflammation
High cortisol state (marginated pool of neutrophils released) |
|
|
What is considered the marginal pool of neutrophils?
|
These are the neutrophils adhesing to the bv and just stay attached. High levels of cortisol releases it into the blood vessel (increasing the count)
Neutrophil Leukocytosis |
|
|
Pt. with bacterial infection has both leukopenia and leukocytosis (neutrophils mainly).
Explain that |
TIME-DEPENDENT
early infections usually leukocytosis. As it progresses and becomes severe (deadly, septic shock like), then it is leukopenia (low neutrophil count) WEIRD |
|
|
Leukocytosis during bacterial infection
Left shift or right? Why? Immature cells have more or less FC receptors?* |
Immature forms (left shift) due to more neutorphils produced quickly.
Immature cells have LESS FC receptors (CD16) |
|
|
What CD are FC receptors?
Are they increased or decreased in immature neutrophils during bacterial infection (leukocytosis) |
CD16
DECREASED FC receptors** |
|
|
Monocytosis
What is it? Common causes? |
Increased circulating monocytes
Common causes: -Chronic inflammation (autoimmune and infections) -malignancy |
|
|
Eosinophila
What is it? Common causes? |
Increased circulating eosinophils
Common causes: Allergic rxns (type I) Parasitic infections Hodgkin lymphoma* |
|
|
In Hodkin's lymphoma you have an increased or decreased Esophilia?
MOA? (hint: why cytokine) |
INCREASED Eosinophila
HL produces IL-5 which increases eosinophils |
|
|
Basophila
What is it? Common causes? |
Increased circulating basophils
Common causes: Chronic Myeloid Leukemia** |
|
|
Lymphocytic leukocytosis
What is it? Common causes? |
increased circulating lymphocytes
Common causes -Viral infections (T-Cell hyperplasia) -Bordetella pertussis infection (Exception to the rule) |
|
|
What organism mainly causes Infectious Mononucleosis?
What is a less common cause? |
EBV infection = most common cause of mono
CMV = less common cause |
|
|
How is EBV transmitted?
What age group is it common in? (hint: you already know about mono!) |
"Kissing disease"
Spread via saliva Common in teenagers |
|
|
Common symptoms of Infectious mono?
|
Fever, malaise, sore throat, swollen/enlarged lymph nodes, BIG spleen
|
|
|
What 3 things does EBV primarily infect?
|
Throat
Liver - resulting in hepatitis with hepatomegaly B cells |
|
|
What cells of the immune system primarily respond to EBV infection?
(hint: all viruses cause this cell to be activated) |
CD8+ T-cells
|
|
|
CD8+ T cell response leads to??
|
Generalized lymphadenpathy due to T-cell hyperplasia in lymph nodes
Splenomegaly due to T-cell hyperplasia in the spleen |
|
|
Where in the spleen is the T-cell hyplerplasia occuring?
|
Periarterial lymphatic sheath (PALS)*
(if you don't know what that is, review Spleen histology; FLashcard coming soon near you!) |
|
|
Normal Spleen Histology?
Red Pulp vs. White Pulp? |
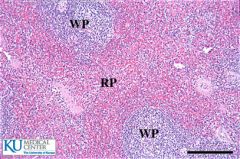
Red Pulp: BV mainly (hence red)
White pulp (actually blue): site of B and T cells |
|
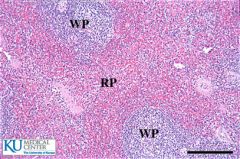
Where is the Periarterial lymphatic sheath?
What is happening here? |
This is the outside area of the white pulp.
T-cell proliferation occurs here |
|
|
Normal Lymph node histology:
Find Cortex, paracortex, medulla (and figure out what grows where) |
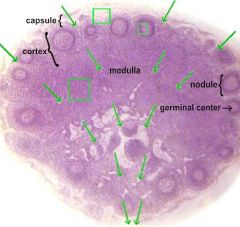
Cortex: B- cells
Paracortex: T-cells |
|
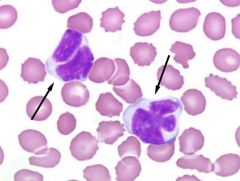
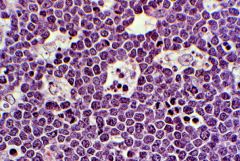
What disease is this?
What cell does it represent? |
Mono
Atypical lympocyte (CD8+ T cell) |
|
|
Monospot test screening or definative diagnosis?
|
Screen test for mono
|
|
|
What are heterophile antibodies? Who produces them? What test detects them?
|
These are weird ABs made against the horse or sheep blood cells when someone is infected with mono.
Monospot test detects them |
|
|
IgM antibodies against sheep/horse RBC are called?
|
Heterophile antibodies
|
|
|
14 yr male pt. has had a fever and has been feeling weak for few days. History suggests a new girlfriend. Physicial exam reveals enlarged posterior cervical lymph nodes, normal size liver, but enlarged spleen. You suggest mono and do a monotest, but it comes back negative. What do you think he has?
|
CMV infection (also causing mono --- same symptoms just caused by different virus).
(whenever you suspect mono but test comes back negative, think CMV!) |
|
|
How do you make a definite diagnosis of EBV?
|
Serologic studies looking for EBV antigens
|
|
|
What are some complications associated with Mono?
|
Increased risk of splenic rupture (b/c it is big)*
Recurrence and B-cell lymphoma (if immunodeficient) b/c the virus stays dormant in the B-cells it infects |
|
|
Acute Leukemia
What is it? |
Neoplastic proliferation of the blasts;
defined as accumulation of >20% of blasts in the BM |
|
|
How does Acute leukemia cause anemia, thrombocytopenia and neutropenia?
|
Increased blasts "crowd out" normal hematopoiesis resulting in decreased production of everything
|
|
|
Why do you get high WBC in acute leukemia?
|
B/c the Blasts (neoplastic) enter blood stream
|
|
|
What do the neoplastic blast cells look like?
|
Blasts are large, immature cells, often with punched out nucleoli
|
|
|
Two divisions of Acute leukemia?
|
Divisions based on whether it is the myleoid linage or lympocytic linage
AML and ALL |
|
|
Acute Lymphoblastic leukemia (ALL)
What is it? |
Neoplastic accumulation of lympoblasts (>20%) in the bone marrow
|
|
|
What marker is used to detect ALL?
|
TdT, a DNA polymerase**
|
|
|
ALL is commonly associated with what disease?
What age? |
Down syndrome
Usually AFTER age 5 |
|
|
2 subdivisions of ALL?
ALL common in what age group? |
B-ALL and T-ALL
usually children |
|
|
Most common type of ALL?
|
B-ALL
|
|
|
B-ALL is usually characterized by TdT+ lymphoblasts that express CD__, CD__ and CD___
|
CD10, 19, 20
(hint: For B-cells, CD are greater then 10) |
|
|
Prognosis of B-ALL is based on?
|
Cytogenetic abnormalities
t(12;21) has good prognosis; more common in children t(9;22) has poor prognosis; adults (philadelphia chromosome) |
|
|
T-ALL is characterized by TdT+ lymphoblasts that express CD__, CD__, etc. markers
|
Markers ranging from Cd2-CD8
(hint: For T cells, CD are less then 10) |
|
|
T-ALL cause a mediastinal mass hence another name is acute lympoblastic LYMPHOMA
T/F? |
TRUE
|
|
|
Acute Myeloid Leukemia (AML)
What is it? |
Neoplastic accumulation of myeloblasts (>20%) in the BM
|
|
|
AML common in what age group?
|
Usually elderly (~55)
|
|
|
AML is characterized by positive cytoplasmic staining for?
|
MPO**
|
|
|
When you stain for Myeloperoxidase (MPO) in AML, crystal aggregates might form. What are these called?
|
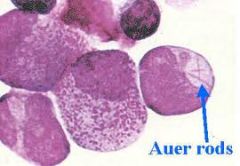
Auer rods
|
|
|
AML subtypes?
(hint: there are many; know the high yield ones -- 3) |
Acute promyelocytic leukemia
Acute monocytic leukemia Acute megakaryoblastic leukemia |
|
|
Acute Promyelocytic leukemia
What is it? MOA (what genetic abnormality)* |
A subtype of AML
t(15;17) which involves translocation of retinoic acid receptor on chom 17 to chrom 15** |
|
|
RAR disruption blocks maturation of myloid and promyelocyte accumulate
What disease is this? What genetic abnormality? |
Acute promyolocytic leukemia (form of AML)
t(15;17) of RAR (needed for maturation) |
|
|
What emergency risk are you at for in pt. with Acute promyelocytic leukemia? Why?*
|
Dissemented Intravascular Coagulation*
APL has many auer rods which increase risk of DIC |
|
|
Tx of APL?
|
ATRA (vitamin A derivative)
Binds to altered receptor and causes the blasts to mature (and die) --> lets the RAR do its function |
|
|
Acute monocytic leukemia
What is it? Common place to infiltrate?* |
Proliferation of monoblasts (form of AML)
Infiltrates gums* (swelling) |
|
|
Acute megakaryoblastic leukemia
What is it? Associated with what? at what age? |
Proliferation of megakaryoblasts (form of AML)
Associated with Downs BEFORE age 5 |
|
|
What two blood cancers associated with Downs?
|
Acute megakaryoblastic leukemia (form of AML) = BEFORE age 5
ALL = AFTER age 5 |
|
|
What is chronic leukemia?
|
Neoplastic proliferation of mature circulating lymphocytes;
usually takes a long time to occur (thus usually adults) |
|
|
Chronic lymphocytic leukemia (CLL)
What is it? |
Neoplastic proliferatoin of naive B-cells that co-express CD5 and CD20
(weird b/c low numbers usually T-cell associated) |
|
|
What is the most common leukemia overall?
|
Chronic Lymphocytic Leukemia
|
|
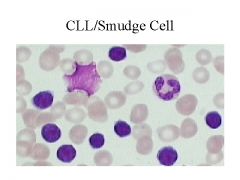
What disease is this?
How do you know? |
Chronic Lymphocytic Leukemia
SMUDGE CELL** |
|
|
Complications of CLL?
|
Hypogammaglobulenima - the B cells don't become plasma cells (increased risk of infection)
Autoimmune hemolytic anemia - if they do become plasma cells, the AB are stupid Transformation to diffuse large B-cell lymphoma |
|
|
Richter transformation
|
CLL turning into diffuse large B-cell lymphoma
|
|
|
Hairy Cell Leukemia
What is it? |
Neoplastic proliferation of mature B cells characterized by hairy cytoplasmic processes
|
|
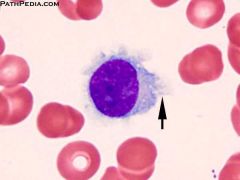
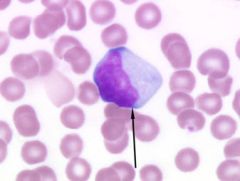
What is this?
|
hair cell leukemia
(The hairy process is what the arrow is pointing at) |
|
|
In hairy cell Leukemia, what are the cells positive for?
|
Tartrate resistant acid phosphatase
|
|
|
2 clinical features of Hairy Cell leukemia
(hint: spleen and BM) |
Splenomegaly and "dry" tap on BM aspiration (due to marrow fibrosis)
|
|
|
Why do you get splenomegaly in Hairy Cell Leukemia (this is weird)
|
Due to accumulation of hairy cells in the red pulp (instead of white)
|
|
|
General features of Chronic leukemia regarding lymph nodes and spleen?
Explain why hairy cell leukemia is an exception |
Splenomegaly (generally WHITE pulp hyperplasia)
Enlarged lymph nodes In Hairy cell, you have no lymph node enlargement and it is the RED pulp |
|
|
Treatment for Hairy cell leukemia?
|
2-CDA (Cladribine) - adenosine deaminase inhibitor (adenosine will accumulate and cells will die)
Excellent response |
|
|
Adult T-Cell Leukemia/Lymphoma (ATLL)
What is it? Associated with what in what areas of the world? |
Neoplastic proliferation of mature CD4+ T cells (like to go to skin).
Associated with HTLV-1 infection; most commonly seen in Japan and Caribean** |
|
|
Clinical features of Adult T-Cell Leukemia/Lymphoma (ATLL)
|
lymphadenopathy, hepatosplenomegly (two things associated with any CL), lytic bone lesions with hypercalcemia
|
|
|
A person with punched-out lesion and you think there is some blood cancer. What is your DDx?
|
ATLL and Multiple Mylemona
|
|
|
Mycosis Fungoides
What is it? |
Neoplastic proliferation of mature CD4+ T cells (like ATLL) but it has distinctive characteristics
(spreads to blood) |
|
|
Clinical features of Mycosis Fungoides
|
Localized skin rash, plaques and nodules (b/c CD4 T cells accumulate in skin);
Also goes into blood stream |
|
|
Pautrier microabcesses
What is it? seen in what disease? |
Neoplastic cells in epidermis = Pautrier microabscesses
Seen in Mycosis Fungoides |
|
|
If the neoplastic CD4 T-cells in Mycosis Fungoides spread to blood stream, what is the disease called?
What are the characteristic cells in blood smear? |
Sezary syndrome
Sezary cells (bunch of lobes in the nucleus) |
|
|
Myeloproliferative Disorders
What is it? |
Neoplastic proliferation of mature cells of the myeloid lineage (eg. too many RBC or platelets)
Old age usually |
|
|
What cells are usually incresaed in Myeloproliferative Disorders?
|
All cells of the myeloid lineage are increased (eg. RBC, neutrophils, Platelets, monocytes).
However we name it based on the dominating one. |
|
|
Complications associated with Myeloproliferative Disorders
|
Increased risk of hyperurecemia and gout due to high turnover
Progress to marrow fibrosis or transformation to acute leukemia |
|
|
Name some Myeloproliferative disorders
|
Chronic Myeloid Leukemia (granulocytes-basophils)
Polycythemia Vera (RBCs) Essential Thrombocythemia (platelets) Myelofibrosis (MK) |
|
|
Chronic Myeloid Leukemia (CML)
What is it? |
Neoplastic proliferation of mature myeloid cells, especially granulocytes (mainly basophils**)
|
|
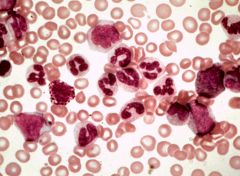
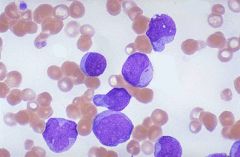
What is this?
|
Chronic Myeloid Leukemia
Lots of lympocytes (those big huge things), especially basophils usually |
|
|
What genetic abnormality is associated with CML?
(hint: city) |
Philadelpha chromosome: t(9;22)
|
|
|
What does the Philadelphia chromosome t(9;22) translocation lead to?
(hint: some kind of fusion) |
BCL-ABL fusion protein
This increases tyrosine kinase activity (increased GROWTH) |
|
|
What can be a complication of CML?
|
Can advance to AML or ALL
(Note: if you are confused as to why it can turn into ALL --> it is b/c the error is in the FIRST step of hemapotosis) |
|
|
How can you differentiate CML from leukemoid reaction (eg. lots of lymphocytes) during infection and stuff?
(random list, be familiar with) |
-Negative Leukocyte Alkaline Phosphatase stain in CML (+ in leukoemoid rxn)
-Increased basophils in CML -Philadelpha chromosome |
|
|
Polycythemia Vera
What is it? |
Neoplastic proliferation of mature myeloid cells, especially RBCs
|
|
|
What mutation do you have in Polycythemia vera?
|
JAK2 Kinase mutation
|
|
|
Clinical features of Polycythemia Vera
(all caused by what?) |
All symptoms caused by blood being viscous (too many RBCs)
Blurry vision headache Increased risk of Venous thrombososis Flushed face due to congestion Itching (due to increased mast cells) |
|
|
Tx. of Polycythemia Vera
|
Phelobotomy
|
|
|
If you don't treat a pt. with Polycyhtemia Vera, what happens?
|
Pt. dies within an yr
|
|
|
How do you differentiate b/w Polycythemia Vera and reactive polycythemia (increased RBC due to some weird stimulus)?
|
In PV, Erythropoietin levels are decreased (negative feedback)
And O2 saturation should be normal (duh --- why would that change) |
|
|
Essential Thrombocythemia
What is it? |
Neoplastic proliferation of mature myeloid cells, especially platelets
|
|
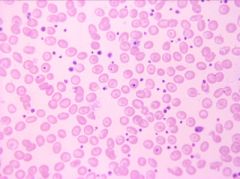
What is this?
|
Essential Thrombocythemia (ET)
little dots = platelets |
|
|
What mutation is associated with Thrombocythemia?
|
JAK2 kinase mutation (just like Polychtemia Vera---RBC)
|
|
|
Symptoms of Essential Thrombocythemia?
|
Either too much bleeding or too much clotting
All depending on if the extra platelets are working (clots) or are defective (leading to bleed) |
|
|
Most Myeloproliferative Disorders have potential complications of hyperurecemia, marrow fibrosis, and acute leukemia transformation EXCEPT?
|
Essential Thrombocyhthemia
|
|
|
Myelofibrosis
What is it? |
Neoplastic proliferation of mature myeloid cells, especialy megakaryocytes
|
|
|
What do megakaryotes produce that leads to marrow fibrosis?
|
produce excess platelet-derived growth factor causing marrow fibrosis (hence the name)
|
|
|
Why do you have increased risk of infection, thrombosis, bleeding and splenomegaly in Myelofibrosis?
|
Due to the excess fibrosis, the BM sucks at making everything. Spleen (and other places) take over, but just aren't good enough :(
|
|
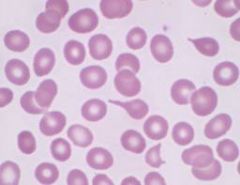
Notice that long RBC.
|
Tear drop cells of Myelofibrosis (the BM sucks at making them right)
Would also see immature granulocytes and immature RBC (with nuclues) b/c Spleen doesn't check whether they mature or not (its stupid) |
|
|
What is Lymphoma and what is it sub-divided into?
|
Neoplastic proliferatoin of lyphoid cells that form a mass;
Divided into non-Hodgkin (60%) and Hodgkin lymphoma |
|
|
Non-hodgkin is further divided into what?
|
Divided based on many things (one being size and type of cell---B or T)
Small B cells (Follicular, Mantle, Marginal), Intermediate (burkitt), Large B cells There are many many more but those are the high yields (mainly B) |
|
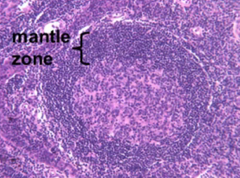
Where is the Follicle?
Where is the Mantle zone? Where would the marginal zone be (if it was there)? |
Follicle is inside the Mantle zone (pink)
Mantle zone is labeled (duh) Marginal zone would be OUTside of the mantle zone |
|
|
Follicular Lymphoma
What is it? |
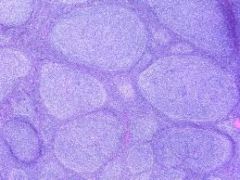
Neoplastic proliferation of small B-Cells (CD20+) that form follicle-like nodules
(lots of follicles - little circle things) |
|
|
What genetic abnormality lead to Follicular lymphoma?
|
t(14;18) trans-location
BCL on chromosome 18 translocated to the Ig heavy chain locus on chromosome 14 (highly expressed) |
|
|
Increased expressoin of BCL2 in Follicular lymphoma leads to what?
|
Inhibits apoptosis, hence the tumor
|
|
|
How do you differentiate Follicular lymphoma from follicular hyperplasia?
|
Lymphoma disrupts normal lymph node structure (spreads everywhere)
Lack of tingible body macrophages in lymphoma BcL2 expression in lymphoma Monoclonality in the lymphoma ( |
|
|
What are tingibile body macrophages?
|
These are just MC which are present in hyperplasia and stuff to clean out the dead cells.
In lymphoma the cells don't die, thus NO MC present. |
|
|
What is Mantle Cell Lymphoma?
|
Neoplastic proliferation of small (CD20) that expands the mantle zone (right outside the follicle)
"adjacent to follicle" |
|
|
What genetic abnormality drives Mantle Cell Lymphoma?
|
t(11;14) trans-location
Cyclin D1 gene on 11 goes to Ig heavy chain locus on chromosome 14. |
|
|
What is the role of cyclin D1? What happens if it is overexpressed (as the case with mantle Cell lymphoma)
|
Cyclin D1 promotes G1/S transition
overexpression leads to cancer (uncontrolled growth!) |
|
|
What is Marginal Zone lymphoma
|
Neoplastic proliferation of small B cells (CD20+) that expands the marginal zone
|
|
|
What is Marginal Zone lymphoma associated with?
|
Associated with chronic inflammatory states
Eg. Hahimoto thyroiditis, Sjogren syndrome, H. pylory gastritis |
|
|
What is MALToma
|
Marginal zone lymphona in mucosal sites
(usually associated with H.pylori) |
|
|
What is Burkitt Lymphoma?
Associated with what virus? |
Neoplastic proliferation of intermediate-sized B cells (CD20+);
associated with EBV |
|
|
Compared to other Non-Hodgkin lymphomas, who (age group) does Burkitt's present in?
|
usually in kids (other ones usually adults)
|
|
|
What are the two forms of Burkitt's lymphoma?
|
African form usually involves jaw
Sporadic form usually involves abdomen |
|
|
What genetic abnormality is associated with Burkitt's lymphoma?
|
t(8;14)
c-myc on chromosome translocated to chromosome 14 (Ig heavy chain); hence heavily expressed, leading to cell growth |
|
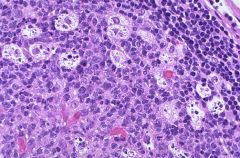
Starry-sky apperance in what disease?
|
Burkitt's lympoma
sky = blue = proliferating B cells starry = white = MC cleaning it up |
|
|
What is Diffuse Large B-Cell lymphoma?
Aggressive or NBD? |
Neoplastic proliferation of large B-cells (CD20) that grow diffusely
Clinically agressive (high grade) |
|
|
What is the most common form of Non-hodgkin lymphoma?
|
Diffuse Large- Bell Lymphoma
|
|
|
How does Diffuse Large B-cell lymphoma arise?
|
Like most, it can come sporadicly.
Or it can come from some low grade lymphoma (eg. follicular) |