![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
177 Cards in this Set
- Front
- Back
|
Name 5 modifiable RF for ischaemic heart disease |
Smoking Obesity Hyperlipidaemia Hypertension Diabetes mellitus Sedentary lifestyle Cocaine use |
|
|
How is family history usually considered positive in ischaemic heart disease |
First degree relative with MI ≤ 55 |
|
|
What may precipitate ischaemic heart diseases (4)? |
Cold weather Heavy meal Anxiety Exercise |
|
|
Characterise the radiation of angina pectoris (4) |
One or both arms Neck Jaws Teeth |
|
|
Name 3 possible mechanisms that may cause ischaemic heart disease. Which is by far the most common? |
Atheroma Aortic stenosis Vasculitis Tachy-arrhythmias |
|
|
What is crescendo angina |
A synonyme of unstable angina, i.e. angina experienced with minimum exercise or at rest. |
|
|
ECG in angina |
Usually normal (possibly signs of previous MI) |
|
|
Is angina an emergency? |
No, but unstable angina is. |
|
|
Outline how you would manage a patient for which you do not know whether angina is stable or unstable. |
Based on whether there is a known CAD diagnosed in this patient. 1) Known CAD and pain typical => No further investigation |
|
|
Define acute coronary syndrome |
Unstable angina or MI (STEMI or NSTEMI) |
|
|
How is acute MI diagnosed? |
Raised troponin + one of: - Ischaemic symptoms - Pathological Q-waves - ST elevation or depression - Past coronary intervention |
|
|
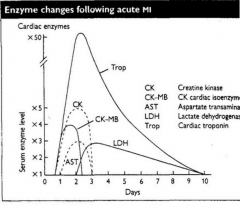
Name four cardiac enzymes that you expect to raise in MI and outline how they evolve. |
|
|
|
Which cardiac enzyme is most useful for the diagnosis of a second MI following a very recent one? |
CK (or CK-MB, even better) |
|
|
Name 4 tissues that may result in raised AST if damaged. |
Liver Heart (cardiac muscle) Skeletal muscle Kidneys RBC Brain |
|
|
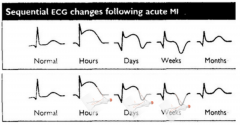
Outline how ECG trace changes with MI over time (from hours, to days, to weeks, to months) |
|
|
|
Besides the central chest pain, name 3 symptoms that can be experienced in MI |
Nausea Sweating Dyspnoea Palpitations |
|
|
Name one presentation of silent MI |
Syncope Pulmonary oedema Epigastric pain and vomiting Acute confusional state Diabetic hyperglycaemic state |
|
|
Name four signs of acute coronary syndrome |
Distress Anxiety Pallor Sweatiness Pulse ➚ or ➘ BP ➚ or ➘ Signs of heart failure Pansystolic murmur (if papillary muscles rupture) |
|
|
What murmur may follow an MI? Why? |
Pansystolic murmur due to papillary muscle dysfunction causing mitral regurgitation or ventricular septal defect |
|
|
What blood tests would you do in someone who has had an MI? |
FBC Glucose Lipid U&E |
|
|
Which 2 troponin are used as cardiac markers? |
T and I |
|
|
When does troponin peak after an MI |
24-48h after (but by 12h it is sufficiently likely raised to be used as a diagnostic marker) |
|
|
Two key investigation results that help with diagnosis and prognosis in a patient with suspected MI |
ST elevation? (worse if ST elevation) Raised troponin? (If it is not, then it is likely unstable angina rather than MI, which has a better prognosis) |
|
|
What is the difference between STEMI and NSTEMI in terms of prognosis? |
STEMI is worse |
|
|
What distinguishes unstable angina from MI? |
Raised troponin in MI |
|
|
What feature mostly drive the choice of management in acute coronary syndrome? |
Presence of ST elevation (NSTEMI and unstable angina are managed similarly) |
|
|
What is the indication for thrombolysis in acute coronary syndrome? |
STEMI with no contraindication |
|
|
Relation between thrombolysis and fibrinolysis |
Fibrinolysis are the drugs used to achieve thrombolysis |
|
|
Initial management of acute coronary syndrome |
MONABASH Morphine IV O2 (if Sats < 94%) Nitrates Aspirin (or more recent antiplatelets) Beta-Blockers ACE-Inhibitors Statins Heparin (or fondaparinux) |
|
|
How does the management of STEMI, NSTEMI and unstable angina differ? |
They all receive the same initial treatment (MONABASH) but differ after. ◾ STEMI ⟹ Coronary angiography + Revascularisation with PCI (if within 2hours of first medical contact) or fibrinolysis (asap but can be up to 24h of onset of symptoms) |
|
|
Relate Percutaneous Coronary Intervention (PCI), CABG, Balloon angioplasty and Percutaneous Transluminal Coronary Angioplasty (PTCA) |
PCI = Balloon angioplasty = PTCA |
|
|
What is the lifelong medications used in a patient who had: - Angina - Unstable angina - NSTEMI - STEMI |
It's the same "BAGS of Aspirin" Beta blockers or verapamil ACE-inhibitor GTN Statins Aspirin |
|
|
What is the indication for PCI in angina? |
STEMI (if available within 2 hours) Others angina that do not resolve with medications |
|
|
What is in two words the rational for using beta blockers in someone who had angina? |
Reduce workload |
|
|
Name 3 complications of uncontrolled angina |
Heart failure Infarction Arrhythmia |
|
|
What sorts of arrhythmias can result from uncontrolled angina? |
Both bradycardia and tachycardia |
|
|
The following may present with chest pain. Explain how they can be distinguished: - Angina - Pericarditis - Myocarditis - Aortic dissection - PE - Oesophageal reflux |
- Angina: radiates to arms, neck, jaw and teeth, relieved by rest, exacerbated by exercise - Oesophageal reflux: brought on by food, alcohol, NSAIDS, relieved by antacids. - PE: SOB, pleural rub, cyanosis, RF - Aortic dissection: tearing pain radiating to the back - Pericarditis: sharp pain, worse lying flat, relieved by sitting forward - Myocarditis: Fever, dyspnoea, fatigue, palpitations, tachycardia |
|
|
Name 4 lifestyle changes that can be attempted in patients following an MI |
- Increase exercise - Change diet (increase oily fish, fruit, vegetables and decrease saturated fat) - Weight loss - Control hypertension - Control diabetes - Encourage smoking cessation |
|
|
Besides lifestyle changes and medications, what other element is part of the treatment of a patient following MI |
Rehabilitation aiming at improving physical and psychological wellbeing—via assessment and treatment of anxiety, structured exercise, education and reassurance. |
|
|
Define heart failure |
Cardiac output inadequate for the body requirement |
|
|
Outline the different mechanisms leading to HF |
Hypoxia ◾︎ Absolute (e.g. coronary atherosclerosis, anaemia, pulmonary disease) ◾︎ Relative (e.g. ventricular hypertrophy) Ventricular dilation HTN, valvular disease |
|
|
Name 3 drug classes that should be avoided in heart failure and explain why. |
Alpha blockers (act as a beta agonist by selectively blocking alpha) Calcium-channel blockers (Negative inotropic) NSAIDs (Salt and water retention and renal impairment) |
|
|
NICE guidelines for the diagnosis of heart failure |
1) ECG or BNP 2) If (1) is normal, then HF is unlikely If (1) is abnormal, then echocardiogram |
|
|
Five features of heart failure on CXR |
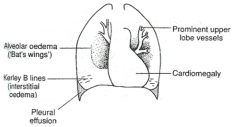
Alveolar oedema (in a ‘bat’s wing’s distribution) B-lines (Kerley) Cardiomegaly Dilated upper lobe vessels Effusion (pleural) |
|
|
Name 4 major criteria for the diagnosis of CHF |
◾︎ Paroxysmal nocturnal dyspnoea ◾︎ Crepitations ◾︎ S3 gallop ◾︎ Neck vein distension ◾︎ Hepatojugular reflux ◾︎ Raised central venous pressure (> 16cmH2O) ◾︎ Weight loss of >4.5kg after 5d of treatment |
|
|
What is the imaging of choice to confirm the diagnosis of HF. What is it useful for? |
Echocardiography Useful to confirm diagnosis, estimate LV performance, investigate the presence of valve disease. |
|
|
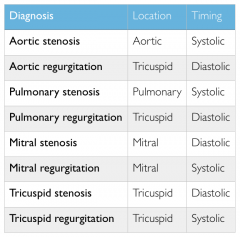
Most regurgitations are heard in tricuspid (think of regurgitation => Flow backwards) except for mitral regurgitation (which is the most common) |
|
|
Outline the physiology of the waves of the JVP |
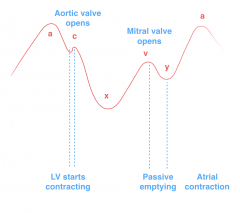
a: atrial systole c: from closure of tricuspid to opening of aortic x: ventricular systole v: opening of mitral valve y: end of passive emptying |
|
|
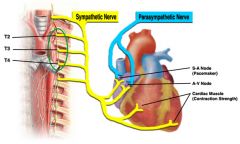
Outline the autonomic nervous supply to the heart |
|
|
|
Name the three effect that the SNS has on the heart function |
Increase HR Increase cardiac contractility Increase Vascular resistance |
|
|
What is congestive cardiac failure? |
Simultaneous L and R heart failure |
|
|
Name two valve diseases that may result in heart failure and outline (in two words) the mechanism. |
Mitral regurgitation: excessive preload Aortic stenosis: excessive afterload |
|
|
Name two diseases that heart failure is associated with in the long term |
Disrrhythmias MI |
|
|
Name the first 3 actions you would initiate in acute heart failure |
Sit patient upright Give 100% O2 (if no underlying lung disease) Monitor and treat arrhythmias |
|
|
Name 3 lifestyle changes that may be beneficial in heart failure |
Reduce salt intake Stop smoking Reduce weight |
|
|
Name 5 drug classes that can be used in heart failure and briefly outline the mechanism of each. |
"DAB DAB" sound of the healthy heart Aldosterone antagonist and ACE-I (or Angiotensin receptor blocker if not tolerated)
2) ACE-I: decrease afterload 3) Angiotensin Receptor blocker: substitute to ACE-I if patient develops cough on ACE-I 4) Beta1-blockers: Reduce cardiac oxygen demand 5) Aldosterone antagonist (spironolactone): decrease preload 6) Digoxin: positive inotropic (symptoms control) |
|
|
What 3 non-pharmacological treatment would you consider in intractable heart failure? |
1) Pacemakers 2) Left ventricular assist device (LVAD) 3) Heart transplant |
|
|
Name 3 causes of arrhythmias that are not cardiac |
Caffeine Smoking Alcohol Pneumonia Drugs (beta2-agonists, digoxin, L-dopa, tricyclics) Electrolyte imbalance Thyroid diseases Phaeochromocytoma |
|
|
A patient is found to have bradycardia. What two drugs would you pay attention to in the drug history? |
Beta-blockers Digoxin |
|
|
What drug would you use in bradycardia and what is the indication for treatment of a bradycardia? |
Treat it HR<40 or if symptomatic Atropine (competitive reversible antagonist of mAChR 1–5) |
|
|
What are the normal values (in ms) on ECG for the following variables: P-wave PR segment QRS complex ST segment T-wave PR interval QT interval |
Remember 3 facts: 1) One heart cycle is 1000ms. 3) The segments before and after the QRS are equal and together are equal to QRS.
P=150ms PR=50ms QRS = 100ms T=350ms From there, other measurements can be calculated. PR interval=P+PR=200ms QT interval=QRS+ST+T=100+50+350=500ms |
|
|
Define broad complex tachycardia |
HR > 100 QRS > 120ms |
|
|
Commonest cause of broad complex tachycardia |
Ventricular tachycardia (VT) |
|
|
Most likely aetiology of ventricular tachycardia |
Ischaemic heart disease damaging the ventricles => Ectopic pacing from the scar tissue |
|
|
What are the two possible presentations of ventricular dysrhythmias? |
1) Asymptomatic 2) Presentation of heart failure (syncope, chest pain, SOB, ...) |
|
|
The following two symptoms can be present in dysrhythmias. State whether they mostly point towards ventricular or supra-ventricular arrhythmias: palpitations, syncope. |
Palpitations => SVT (e.g. AFib) Syncope => Mostly VT (since in SVT, the ventricles will pump more or less hard to compensate for the difference in rhythm) |
|
|
Impact of hyper and hypokalaemia on ECG trace |
Hyperkalaemia Wide QRS - Tall T Hypokalaemia Small T - U wave |
|
|
Impact of hyper and hypomagnesaemia on ECG trace |
Same as with K Hypermagnesaemia Wide QRS - Tall T Hypomagnesaemia Small T - U wave |
|
|
Impact of hyper and hypocalcaemia on ECG trace |
Remember that L-type Calcium channels close only when enough calcium ions have crossed them. Hypercalcaemia Short QT Hypocalcaemia Long QT |
|
|
Impact of hyper and hyponatraemia on ECG trace |
No effect |
|

|
Ventricular tachycardia |
|

|
Ventricular fibrillations |
|
|
Name 3 causes of wide complex tachycardia |
Ischaemia Wolff-Parkinson-White syndrome Sodium-channel blocking agent (e.g. TCA) |
|
|
Name one electrolyte imbalance which may cause wide complex tachycardia |
Hyperkalaemia/Hypermagnesaemia |
|
|
Name one drug that may cause wide complex tachycardia |
Sodium-channel blocking agent (e.g. TCA) |
|
|
What is the pathological difference between ventricular tachycardia and ventricular fibrillation? |
In VF, different spots in the ventricles generate potentials creating a disorganised activity. |
|
|
What should you do immediately with a patient with ventricular tachycardia (even before initiating treatment)? |
Connect to cardiac monitor and have a defibrillator at hand. |
|
|
Management of VFib and VT (explain the MOA or drugs you name) |
VFib – Defibrillation VT with cardiac arrest – Defibrillation |
|
|
Distinguish defibrillation and cardioversion in their principles and indications |
Defibrillation Asynchronised DC shock that can be used without a heart beat to leverage. Indicated in: VFib and Pulseless VT Synchronised shocks during QRS complexes Indicated in: SVT, AFib, AFlutter, VT with pulse |
|
|
True or false: amiodarone should be stopped as soon as VT is over. |
False, amiodarone may need to maintained to avoid recurrence |
|
|
What non-pharmacological interventions should be considered in a patient with VT? What are their indications? |
To avoid recurrence: Implanted cardiac defibrillator In refractory cases: Radiofrequency ventricular tachycardia ablation |
|
|
Name 4 broad aetiologies of AFib and an example of each |
Affecting the atrial tissues Ischaemia Increasing the stress on atria Hypertension Hart failure PE Mitral stenosis Mitral regurgitation Pneumonia Metabolic causes Hypokalaemia/Hypomagnesaemia (think of hyper as causing VT and hypo as causing SVT) Caffeine Alcohol Post-op Idiopathic |
|
|
How do presentations of AFib and AFlutter differ? |
They don't (asymptomatic or dyspnoea, palpitations, chest pain, faints) |
|
|
Distinguish the ECG traces of AFib and AFlut |
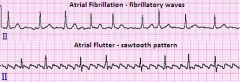
AFib: No P, Irregular QRS
|
|
|
Name 3 blood tests that would help determine the cause of AFib |
TSH Troponin U&E (K and Mg) |
|
|
3 lines of management in a patient with acute AFib |
1. Cardioversion (electrical or chemical–amiodarone or flecainide) 2. Rate control: Beta blockers (bisoprolol) or Ca-channel blocker (verapamil) |
|
|
Risk and indications for cardioversion in AFib |
Risk: thromboembolism Indications: Haemodynamically unstable (benefit outweigh the risk) or AFib < 48h (risk of thrombus is lower). If the patient is haemodynamically stable, then cardioversion should be deferred by 4 weeks during which anti-coagulants can be initiated. |
|
|
What is the risk of verapamil use in AFib? |
If the patient is in heart failure, verapamil may further worsen the heart failure due to its negative inotropic property. Diltiazem is therefore usually preferred as a Ca channel blocker. |
|
|
What metabolic abnormality may predispose to AFib? |
Hypokalaemia/Hypomagnesaemia |
|
|
Name two elements of social history that are important to ask to elicit risk factors for AFib |
Caffeine Alcohol |
|
|
Name 3 elements of the past medical history that are important to elicit risk factors for AFib |
Previous heart surgery (Post-op AFib) Hypertension Previous MI/ACS PE Mitral disease Causes of hypokalaemia (Conn's, Cushing's, Beta agonists, loop and thiazide diuretics) |
|
|
Name 2 drugs that are important to ask about in the drug history to elicit risk factors for AFib |
Beta agonists (drive K into cells => hypokalaemia) Loop and thiazide diuretics (looses K) |
|
|
How do we assess whether a patient that has AF needs to be anticoagulated? |
CHADS-VASc score |
|
|
Effect of hypertension on mortality: what fraction of vascular deaths are related to HTN and how many deaths does it cause? |
50% of all vascular deaths 8M deaths a year |
|
|
Why is HTN difficult to define? |
Because the distribution in the population is skewed normal |
|
|
Name 4 signs that can be elicited on examination and may point to the cause of HTN |
Endocrine Signs of hypercalcaemia (hyperPTH) Renal Oedema (glomerulonephritis) Cardiac Radiofemoral delay (coarctation) Other Distended abdomen (pregnancy ;-)) |
|
|
Name 3 signs that can be elicited on examination and may indicate the presence of end-organ failure in HTN |
Displaced apex beat (Cardiac failure) Focal neurological deficits (Cerebrovascular failure) Hypertensive retinopathy (Retinal failure) Peripheral and pulmonary oedema (Renal failure) |
|
|
Name 2 bedside tests (and the corresponding results) that can be done to indicate the presence of end-organ failure in HTN |
ECG – LV hypertrophy Urinalysis – Protein +++ and blood +++ |
|
|
What proportion of HTN is primary? |
95% |
|
|
Name 5 modifiable RF for HTN |
Hyperlipidaemia Alcohol Smoking Lack of exercise Sleep apnoea Obesity High salt intake |
|
|
What is the treatment goal in HTN in the general population and in diabetics |
140/90 130/80 in diabetic |
|
|
Whom should we treat for HTN |
1) Clinical BP > 180/110 2) Clinical BP > 140/90 with: 2.1) ABPM (ambulatory BP monitor) > 150/95 2.2) ABPM > 135/85 with CV risk > 20% at 10yrs or with end-organ damage 2.3) Clear end-organ damage |
|
|
What are the four elements of hypertensive retinopathy |
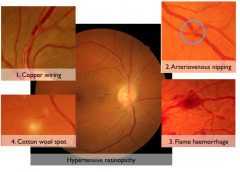
Note: Silver/Copper wiring is not exactly as illustrated |
|
|
Significance of cotton wool spot on fundoscopy? |
Damage to nerve fibers (seen in hypertensive and diabetic retinopathy) |
|
|
What tool is used to measure BP |
Sphygmomanometer |
|
|
Name three anti-hypertensive that you would strongly consider in a patient with a comorbidity of heart failure. |
AB*D (Not C as they are negatively inotropic) ACE-I or Angiotensin receptor blocker Beta blockers Thiazide diuretics |
|
|
Name one anti-hypertensive that you would strongly consider in a patient with a comorbidity of CKD |
ACE-I or Angiotensin receptor blocker |
|
|
What antihypertensives would you not give to a pregnant women? |
ACE-I and Angiotensin receptor blocker |
|
|
Which antihypertensive would you not give to a patient with gout? |
Thiazide diuretics |
|
|
What 3 classes of drugs are mostly used in the general population (i.e. no specific comorbidity) with HTN? |
ACD ACE-inhibitor or Angiotensin receptor blocker Calcium channel blocker Diuretics (thiazide) |
|
|
Outline the steps of anti-hypertensive algorithm. |
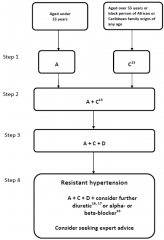
A: ACE-I or ARB C: CCB D: Thiazide diuretics |
|
|
Name one thiazide diuretics used in HTN |
Indapamide or chlortalidone (Not benreoflumethiazide) |
|
|
Define malignant hypertension |
Rapid rise in BP leading to vascular damage |
|
|
What is the pathological hallmark of malignant hypertension? |
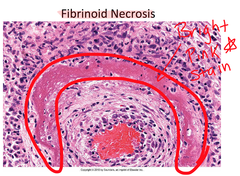
Fibrinoid necrosis |
|
|
Name one sign and one symptom of malignant hypertension |
Sign: bilateral retinal haemorrhage Symptom: headache and visual disturbance |
|
|
Prognosis of malignant hypertension if treated and if not. |
Treated: 90% survival at 1yr Untreated: 90% death at 1yr |
|
|
Name three emergencies that may be caused by malignant hypertension |
(Think of the end-organ failure minus the retinal one) Acute renal failure Acute heart failure Encephalopathy |
|
|
How quickly should malignant hypertension be traeted? |
Over days (not hours as it would increase the risk of stroke) |
|
|
How should malignant hypertension be treated? |
Bed rest Choice of hypotensive: typically atenolol or long-acting calcium channel blockers |
|
|
Two weeks after having initiated treatment for HTN (it was 170/110), you patient returns and a BP measurement is taken. It indicates 165/100. Should you increase the dose? |
No, most hypotensives take 4-8 weeks to have full efficacy. Furthermore, BP fluctuates => Measure several times over a longer period to assess efficacy |
|
|
Besides hypotensives what other two drugs may be considered in a patient with hypertension? |
Statins (based on QRISK) Aspirin (if age > 55) |
|
|
Name one tool used to assess the risk of cardiovascular events (MI or stroke) at 10 years. |
QRISK |
|
|
Outline one system in the body that regulates BP |

|
|
|
What triggers renin production (3)? |
Pressure of afferent arterioles ➘ (this explains why renal stenosis causes HTN) NaCl level in macula densa ➘ Activation of β1-adrenergic receptors (this is how SNS increases BP on top of vasoconstriction) |
|
|
How does renal stenosis cause HTN? |
Arterial stenosis => Low BP distal to the stenosis => Low BP in afferent arterioles => Renin secretion |
|
|
What is the most likely aetiology of aortic stenosis? Name 2 other aetiologies |
Senile calcification (50%) Bicuspid valve (35%) Rheumatic fever |
|
|
Classic triad of symptoms of aortic stenosis |
"Poor blood supply due to HF" Angina Syncope Heart failure |
|
|
Name 4 signs of aortic stenosis on examination |
Slow rising pulse Narrow pulse pressure Ejection systolic murmur radiating to carotids Heaves Quiet heart sounds |
|
|
Prevalence of bicuspid valve |
2% of males 1% of females |
|
|
Most likely aetiology of aortic stenosis in a 45 years old? |
Bicuspid valve |
|
|
What proportion of all aortic stenoses is caused by bicuspid valve? |
35% |
|
|
How is aortic stenosis diagnosed and how is prognosis made? |
Echocardiogram for both. It measures: 1) Valve area (< 1cm2 => Severe) 2) Velocity and hence calculate peak gradient (> 50mmHg => Severe) |
|
|
Name three complications of aortic stenosis |
Ventricular arrhythmia Left ventricular hypertrophy Ischaemia Heart failure |
|
|
What are the RF for aortic stenosis? |
The same as those for coronary artery disease: Hypertension Age Male Hyperlipidemia Diabetes mellitus Smoking Metabolic syndrome End-stage kidney disease |
|
|
What are the common presentations of aortic regurgitation? |
"Think of blood flowing backwards" Exertional dyspnoea Orthopnoea Paroxysmal nocturnal dyspnoea |
|
|
Five causes of aortic regurgitation |
Acute Infective endocarditis Ascending aortic dissection Chronic Rheumatic fever (endocarditis) Hypertension Marfan's syndrome RA, SLE Syphilis |
|
|
What two valve diseases is Marfan's syndrome at risk of? |
Aortic regurgitation Mitral regurgiataion |
|
|
Name 4 signs of aortic regurgitation on examination |
Collapsing pulse Wide pulse pressure Displaced apex beat High pitch early diastolic murmur (best heard in expiration with patient sitting forward) Pulmonary crepitations |
|

A 65 year old patient presents with dyspnoea. On further questioning, he has nocturnal paroxysmal dyspnoea and exertional dyspnoea. On examination, there is a early diastolic murmur and BP is 140/70. His chest X-ray is displayed. What is the diagnosis? |
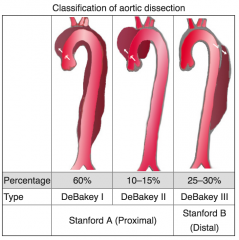
Aortic dissection (Type A) causing aortic regurgitation |
|
|
Name two signs of aortic regurgitation that can be elicited on auscultation |
Early diastolic murmur (best heard in expiration with patient sitting forward) Pulmonary crepitations |
|
|
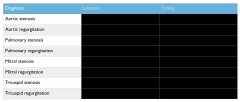
Which valve disease may lead to the following complications: - Arrhythmias - Ischaemia - Left ventricular dilation - Left ventricular hypertrophy - Left atrial dilation - Heart failure |
- AFib: Mitral stenosis, Mitral regurgitation - Ventricular arrhythmias: Aortic stenosis - Ischaemia: Aortic stenosis, Aortic regurgitation - Left ventricular dilation: Aortic regurgitation - Left ventricular hypertrophy: Aortic stenosis, Aortic regurgitation, Mitral regurgitation - Left atrial dilation: Mitral regurgitation - Heart failure: Aortic stenosis, Mitral regurgitation, Aortic regurgitation |
|
|
Name one variable that is a significant factor in the prognosis of aortic regurgitation. |
SBP (Elevated => Worse prognosis) Ejection fraction |
|
|
Outline the vicious circle that operates in aortic regurgitation |
SBP high => Aortic regurgitation => Stroke volume increases => Hypertrophy => SBP increases |
|
|
Most likely cause of mitral stenosis |
Rheumatic heart disease |
|
|
Presentation of mitral stenosis |
Dyspnoea Fatigue Palpitations Chest pain Emboli Haemoptysis (Pulmonary hypertension) Symptoms due to compression of LA on adjacent structure: dysphagia, hoarseness |
|
|
Which valve disease may present with haemoptysis |
Mitral stenosis due to pulmonary hypertension |
|
|
Name 4 signs of mitral stenosis on examination |

AF Tapping apex beat Loud S1 Low pitch rambling mid diastolic murmur Malar flush on cheecks (due to decrease cardiac output) Pulmonary crepitations (due to lung oedema) |
|

What valve disease? |
Mitral stenosis (Malar flush on cheeks) |
|
|
Which valve disease is a RF for systemic emboli? |
Mitral stenosis |
|
|
Which valve disease is a RF for subacute infective endocarditis? |
Mitral stenosis |
|
|
What explains the dysphagia in mitral stenosis? |
Compression of the oesophagus by the enlarged left atrium |
|
|
Three RF of mitral stenosis |
Those of rheumatic fever: Strep pyogenes infection Poverty Malnutrition |
|
|
Name 5 causes of mitral regurgitation |
➙ Rheumatic heart disease ➙ Endocarditis ➙ Ruptured papillary muscles or chordae tendinae ➙ Mitral valve prolapse ➙ Dilation of heart due to ischaemia ➙ Marfan's |
|
|
Presentation of mitral regurgitation |
Dyspnoea Fatigue Palpitations |
|
|
Name 3 signs of mitral regurgitation on CXR |
Enlarged left atrium Hypertrophied left ventricle Mitral valve calcification Pulmonary oedema |
|
|
What is mitral valve prolapse? What other valve disease is it associated with? |
Common (5%) congenital abnormality of the mitral valve which may lead to mitral regurgitation |
|
|
Two complications of prosthetic valves |
Risk of endocarditis Risk of thrombosis (needs anticoagulants) |
|
|
Name one neurological complication of endocarditis |
Septic embolus from initial thrombus formed onto inflamed valve |
|
|
How do patients with endocarditis present? |
Fever and sepsis + Signs of the valve disease affected |
|
|
Which valve is most likely affected by endocarditis in the general population? In IV drug users? |
Mitral (same as for Rheumatic fever) (Tricuspid in IV drug users) |
|
|
8 signs and symptoms of endocarditis |
FROM JANE Fever Roth spots (retinal haemorrhage) Osler nodes Murmur Janeway lesions Anaemia (of chronic disease—normocytic) Nail haemorrhage (splinter) Emboli |
|
|
Distinguish acute and subacute endocarditis in terms of: - Most likely organism - Aetiology (RF) |
Acute Staph. aureus Usually enter via the skin due to: - Wound infection - Dermatitis - IV drug use Subacute Strep viridans Usually develop directly on the valve due to: - Aortic or mitral valve disease - Coarctation of the aorta - Congenital structural defect (PDA, VSD) - Prosthetic valves |
|
|
A patient who received a prosthetic valve yesterday now presents with a new murmur and fever. What is the likely pathogenesis? |
Endocarditis due to infection of the valve during surgery |
|
|
A patient who received a prosthetic valve one year ago now presents with a new murmur and fever. What is the likely pathogenesis? |
Endocarditis due to haematogenous spread of an bacterial focus (not necessarily pathogenic at the primary site). |
|
|
What typically causes infective endocarditis: sepsis or bacteraemia? |
Bacteraemia: the primary presence of bacteria in the blood needs not be pathogenic. It is usually the fact that the immunity of the valve to be infected is lessen (e.g. prosthetic valve). Example: When we chew, bacteria enter our blood and may cause endocarditis in a patient at risk. |
|
|
Name 6 pathogens that are likely the cause of infective endocarditis. |
Strep. viridans (#1) Staph aureus (if wound infection, post-op, etc.) Enterococcus (e.g. E. faecalis) HACEK (Gram -ve bacteria): Haemophilia, Actinobacillus, Cardiobacterium, Eikenella, Kingella |
|
|
How is endocarditis diagnosed? |
Duke criteria 2M or 1M/3m or 5m 1) Positive blood culture (2/3 or N/2N if N>3) 2) Endocardium involvement (echocardiogram or new valve regurgitation) RF (cardiac lesion or IV drug use) Fever >38°C Vascular signs Positive blood culture Positive echocardiogram |
|
|
Characterise the pain experienced in pericarditis |
Central chest pain worse on inspiration or lying flat and relieved by sitting forward |
|
|
Most likely aetiology of pericarditis |
Dressler's syndrome post MI (2-10weeks) Myocardial injury causes the formation of autoantibodies against heart muscle |
|
|
How long after an MI does pericarditis usually occur? |
2-10 weeks |
|
|
Treatment of post-MI pericarditis |
Steroids |
|
|
A patient who has sustained an MI a month ago presents to A&E with central pleuritic chest pain. He finds that sitting forward relieves the pain. A) What is the likely diagnosis and aetiology? B) Name one sign that you could try and elicit on examination. C) You worry that your diagnosis in A may be wrong and that it may be a recurrent MI. What test would you order to rule it out? |
A) Pericarditis secondary to MI (Dressler's) B) Pericardial friction rub or signs of pericardial effusion or cardiac tamponade. C) ECG (cardiac enzymes may be raised in pericarditis) – see other question for the difference of ECG between MI and pericarditis. D) The first group of signs was compatible with pericardial effusion. The second group (BP and HR) is compatible with cardiac tamponade which occurs when pericardial effusion reaches the stage where the accumulation of pericardial fluid impairs ventricular filling and hence cardiac output. F) Anticoagulants (e.g. warfarin) |
|
|
How can pericarditis and MI be distinguished? |
ECG (Cardiac enzymes may be elevated in pericarditis) 1) ST depression in a lead other than AVR or V1? STEMI |
|
|
Name the organisms that may cause pericarditis |
CHIME viruses Coxscackie HIV Influenza Mumps |
|
|
Where does the infection come from in infective pericarditis (2) ? |
Primary infection Secondary (to infection elsewhere) |
|
|
What preventive measure is used for patients at risk of infective endocarditis? |
Patient advice: 1) Explain why prophylactic antibiotics are no longer used. 3) Symptoms of infective endocarditis and when to seek expert advice 4) The risk of undergoing invasive procedure including piercing and tattooing |
|
|
What electrolyte would you measure in someone with hypertension and why? |
Calcium to check for primary hyperparathyroidism as a cause |