![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
88 Cards in this Set
- Front
- Back
|
Significance of raised conjugated/unconjugated bilirubin in the blood |
Pre-hepatic failure – Raised unconjugated Haemolytic anaemia Trauma Gilbert’s Hepatic – Raised unconjugated and conjugated Hepatitis Drugs Alcohol Post-Hepatic – Raised conjugated Primary biliary cirrhosis Cholestasis Primary sclerosing cholangitis |
|
|
Differentiate the following presentations: Biliary colic Peptic ulcers Crohn's disease Ectopic pregnancy Appendicitis Referred pain from chest disease |
Biliary colic Colicky pain, radiates to scapula, no fever, WCC normal Peptic ulcers Pain related to meals (either just before or just after) Heartburn Worse in the early morning Possibly anaemia, haematemesis and melaena Crohn's disease Chronic diarrhoea Extra-intestinal symptoms Weight loss Appendicitis Pain moving Constipation Low grade fever Ectopic pregnancy Similar to appendicitis => Need for a pregnancy test Referred pain from chest disease Look for a chest disease |
|
|
Name 6 differential for abdominal pain |
Biliary colic Peptic ulcers Crohn's disease Ectopic pregnancy Appendicitis Referred pain from chest disease |
|
|
Outline the timeline of biliary colic |
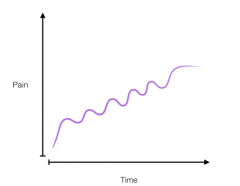
|
|
|
What are the physical signs of biliary colic? |
Usually none (perhaps some non-specific ones related to pain itself) |
|
|
What is an ectopic appendix? How does it present? |
An appendix that is not in its expected orientation (e.g. rotated). |
|
|
What causes chronic cholecystitis? |
1. Repeated episodes of acute cholecystitis 2. Repeated episodes of infection Both cause thickening andfibrosis of gallbladder. |
|
|
Besides gallstones, what may cause cholecystitis? |
Infection |
|
|
Relate non-alcoholic fatty liver disease (NAFLD) and non-alcoholic steatohepatitis (NASH) |
NASH is an extreme form of NAFLD |
|
|
3 most common causes of cirrhosis (and another 3) |
Most common Chronic alcohol abuse Chronic viral hepatitis (Hep B and Hep C) Non-alcoholic steatosis Others Non-alcoholic steatohepatitis Autoimmune Primary biliary cirrhosis (♀) Primary sclerosing cholangitis (♂) Autoimmune hepatitis Genetic Haemochromatosis (iron overload) Alpha1-Antitrypsin deficiency Wilson's disease |
|
|
Name one sign of cirrhosis elicited on palpation |
Early stage: hepatomegaly Later: shrinkage |
|
|
Significance of IgG raised in acute Hep A |
Patient has been exposed to HAV before (Remember "G-General", "M-Moment") |
|
|
Diagnosis of Hep A |
Hep A IgM |
|
|
Incubation period for HAV, HBV and HCV |
HAV 2-6 weeks HBV 1-6 months HCV 2-6 weeks |
|
|
Treatment for Hep A |
No chronic phase => supportive treatment (fluid, anti-emetics or nothing) |
|
|
What non-hep virus can cause acute hepatitis |
EBV, CMV |
|
|
Where is Hep B prevalent? |
Africa, North Canada, North part of South America, South-East Asia |
|
|
Structure of the Hep B virus |
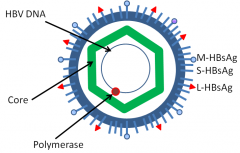
|
|
|
Diagnosis of Hep B infection |
Hep B surface antigen (HBsAg) Hep B core antigen (HBcAg) Virus count |
|
|
Significance of Anti-HBs raised |
Vaccination or cleared infection |
|
|
Significance of Anti-HBc raised |
Cleared infection (not vaccination) |
|
|
Transmission of HBV |
Body fluids (sex, blood, IV drug) and vertical (from mother) |
|
|
What biochemical test may differentiate acute from chronic Hep B infection? |
Anti-HBc |
|
|
Significance of raised HBsAg and raised HBeAg |
Acute on chronic hepatitis B infection |
|
|
Risk factor for acute Hep B infection |
IV drug, blood products, sexual, homosexual, infected mum |
|
|
What Hep viruses do we have vaccines for? |
A and B |
|
|
Treatment of HBV |
Supportive Trace contacts (sexual, other drug users, children) and vaccinate them IFN alpha Oral antiviral therapy (entecavir, tenofovir) |
|
|
How likely is acute liver failure to develop in patients with viral acute hepatitis? |
Unlikely |
|
|
What are the phases of Hep B infection? |
Incubation (high virus, no damage) Clearance (HBeAg positive, high ALT) Low virus carrier (Anti-HBe positive, normal ALT) Reactivation phase (Anti-HBe positive, high ALT) |
|
|
Patients with signs of hepatitis. Blood tests reveal Anti-HBe positive and high ALT. Likely explanation? |
Reactivation phase of HBV infection |
|
|
In what phase of HBV infection do we give treatements? |
Phase 2 (Clearance) and 4 (reactivation) |
|
|
Name two drugs that can be given for HBV? How long should patient take them? |
Entecavir, tenofovir -> Taken for up to 20 years (because of reactivation) |
|
|
Transmission of HCV |
Blood products (transfusion, IV drug, healthcare needles not sterilised), sexual transmission is very rare |
|
|
Diagnosis of Hep C |
IgG test Virus load (only chronic so no acute presentation) |
|
|
When do patients with HCV infection presents? |
Usually when cirrhosis develops, possibly triggered by alcohol |
|
|
Advise given to patients with HCV |
Limit alcohol intake, do not share razors, normal lifestyle |
|
|
Complications of HCV |
Liver failure and death |
|
|
Treatment of HCV |
New revolutionary treatments with 90% cure rates, given orally for 8-12 weeks (£80,000) |
|
|
Patient with acute viral hepatitis but negative hep A IgM and negative HBsAg and hep B core IgM. Likely cause? |
EBV, CMV, Hep E |
|
|
Compare ALT, AST, ALP, γGT, Bilirubin and urine bilirubin in hepatitis and obstruction |
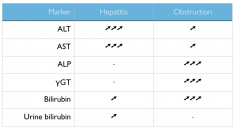
|
|
|
Name 3 symptoms of ascending cholangitis |
Charcot's triad Jaundice RUQ pain Fever and Rigor |
|
|
Outline the possible outcomes of Hep C infections |

|
|
|
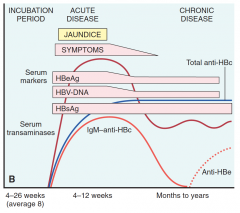
Outline the possible outcomes of Hep B infections |

|
|
|
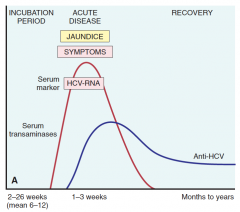
How do ALT, serology and symptoms evolve in acute Hep C which progresses to chronic Hep C? |
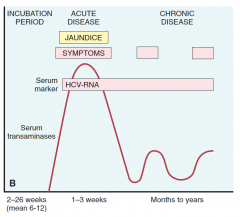
|
|
|
How do ALT, serology and symptoms evolve in acute Hep C which resolve? |
|
|
|
How would LFT, HBsAg, HBeAg, Anti-HBs, Anti-HBe, Anti-HBc IgM and Anti-HBc IgG in incubation? |
HBsAg + HBeAg + Not yet any immunology against it |
|
|
How would LFT, HBsAg, HBeAg, Anti-HBs, Anti-HBe, Anti-HBc IgM and Anti-HBc IgG in acute infection? |
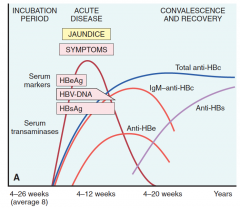
LFT ➚➚➚ HBsAg + HBeAg - (early) | + (late) Anti-HBe - (early) | + (late) Anti-HBc IgM + Anti-HBc IgG - |
|
|
How would LFT, HBsAg, HBeAg, Anti-HBs, Anti-HBe, Anti-HBc IgM and Anti-HBc IgG in chronically infected? |
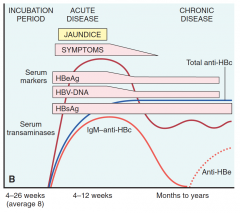
Note: the difference between chronically infected and carrier is that in chronically affected there is active replication so HBeAg + and Anti-HBe - while the converse is true for carriers) LFT ➚ HBsAg + (there is an active infection) HBeAg + (there is an active replication) Anti-HBs - (otherwise there wouldn't be active infection) Anti-HBe - Anti-HBc IgM - (at this stage, the first immune response is over) Anti-HBc IgG + (the long-term response is on) |
|
|
How would LFT, HBsAg, HBeAg, Anti-HBs, Anti-HBe, Anti-HBc IgM and Anti-HBc IgG in carriers? |
Note: the difference between chronically infected and carrier is that in chronically affected there is active replication so HBeAg + and Anti-HBe - while the converse is true for carriers) LFT ➚ HBsAg + (there is an active infection) HBeAg - (there is no active replication) Anti-HBs - (otherwise there wouldn't be active infection) Anti-HBe + (otherwise there would be active replication) Anti-HBc IgM - (at this stage, the first immune response is over) Anti-HBc IgG + (the long-term response is on) |
|
|
Significance of raised HBeAg |
Active viral replication. If it remains high for long, it is a sign of conversion to chronic Hep B infection. |
|
|
Significance of raised Anti-HBe |
Acute infection has peaked and is on the wane |
|
|
How would LFT, HBsAg, HBeAg, Anti-HBs, Anti-HBe, Anti-HBc IgM and Anti-HBc IgG in vaccinated? |
Only Anti-HBs is positive |
|
|
How are Anti-HBc IgG and Anti-HBc IgM measured? |
Anti-HBc IgM is measured directly Anti-HBc IgG is inferred from total Anti-HBc and Anti-HBc IgM |
|
|
Transmission of HAV, HBV and HCV |
HAV Ingestion of contaminated water andfoods and is shed in the stool for 2 to 3 weeks before and1 week after the onset of jaundice. HBV Body fluids (sex, blood, IV drug) and vertical (from mother) HCV Blood products (transfusion, IV drug, healthcare needles not sterilised), sexual transmission is very rare |
|
|
Presentation of Hep A, Hep B and Hep C |
Hep A Mild (jaundice, fever, malaise) or asymptomatic Rarely fulminent (in adults) Hep B More severe than Hep A: arthralgia (pain in joint) and urticaria Hep C Mild or asymptomatic early infection Chronic: Silent (most), cirrhosis (25%) of whom 4% develop hepatoma |
|
|
How long does Hep A take to resorb? |
5-20 weeks |
|
|
Type of virus of HAV, HBV and HCV |
HAV: ssRNA HBV: dsDNA HCV: ssRNA |
|
|
Frequency of chronic infection due to HAV, HBV and HCV |
HAV – Never HBV – 10% HCV – 80% |
|
|
How are we immunised against HAV, HBV and HCV? |
HAV – Inactivated protein HBV – Deactivated HBsAg (active) or Anti-HBs (passive for post-exposure) HCV – None |
|
|
LFT in Hep A |
AST and ALT rise |
|
|
What is the infectious agent in HBV? |
HBsAg (this explains why positive HBsAg implies ongoing symptoms) |
|
|
Name 2 complications of Hep B |
Chronic hepatitis and cirrhosis Hepatocellular carcinoma |
|
|
What is an hepatoma? |
Synonymous of hepatocellular carcinoma |
|
|
Name one virulence factor of HCV |
Poor fidelity of RNA replication => Many variants in a single organism |
|
|
Most likely cause of death in pt with advanced cirrhosis? |
Rupture oesophageal varices |
|
|
Define alcoholic liver disease |
Combination of Fatty liver disease Alcoholic steatohepatitis Cirrhosis |
|
|
Clinical presentation of alcoholic liver disease |
Steatosis ⇒ Hepatomegaly Hepatitis signs and symptoms Cirrhosis ⇒ Silent or signs of complications (see question of cirrhosis presentation) |
|
|
How does cirrhosis present clinically? |
Three possibilities A) Silent B) Features of portal hypertension (ascites, oesophageal varices, caput medusa, ...) C) Features of liver failure (oedema, coagulopathy, encephalopathy) |
|
|
Among the 3 diseases of alcoholic liver disease, which one is the first to occur? |
Steatosis (fatty liver) |
|
|
What two conditions do patients with cirrhosis die of? |
Hepatic failure => oesophageal varices Hepatocellular carcinoma |
|
|
What is non-alcoholic fatty liver disease associated with (3)? |
Obesity Dyslipidaemia Diabetes |
|
|
Outline the pathological features of cirrhosis |
Nodules of regenerating hepatocytes surrounded by broad bands of fibrous tissues. |
|
|
Autopsy of the liver reveals nodules of regenerating hepatocytes surrounded by broad bands of fibrous tissues. What is the process? |
Cirrhosis |
|
|
Name 3 blood test results that you expect in early stages of cirrhosis and 3 in later stages |
Early (hepatocyte damages) AST raised ALT raised ALP raised GGT raised Late (synthetic function impaired) Albumin decreased PT raised Late (spleen engorgement) Platelet decreased WCC decreased |
|
|
Name 3 lines of management that are general (i.e. not related to a specific aetiology or presentation) of cirhhosis |
Maintain good nutrition Avoid alcohol Avoid NSAIDs, sedatives and opiates |
|
|
How would you treat ascites |
Bed rest Fluid restriction Low salt Spironolactone Therapeutic paracentesis may be tried |
|
|
Name 2 indications for liver transplant and 2 contraindications. |
Indications - Advanced cirrhosis (only some aetiologies including the most common ones, the genetic and autoimmune ones but not NASH) - Hepatocellular cancer Contraindications Non-compliance with drug therapy Systemic sepsis Extrahepatic malignancy |
|
|
Distinguish two types of liver failure based on timing. |
Acute (affecting a previously healthy individual) Acute-on-chronic (affecting an individual with an underlying liver disease) |
|
|
What are the causes of liver failure? |
Acute-on-chronic The same as those of cirrhosis Acute Paracetamol overdose Amanita phalloides (mushroom) toxins |
|
|
Relate cirrhosis and liver failure |
Cirrhosis is a pathology (Nodules of regenerating hepatocytes surrounded by broad bands of fibrous tissues) that usually accompanies acute-on-chronic liver failure. |
|
|
Name 6 common signs of liver failure and explain their pathogenesis. Outline which are general to liver failure and which are specific to a specific aetiology. |
General Jaundice – Bilirubin is no more excreted and is present in the blood Encephalopathy – Ammonia is no more cleared and passes into the brain where it is taken up by astrocytes causing oedema Asterixis – Due to encephalopathy Signs of chronic liver disease Oedema – Low albumin Bruises – Low clotting factors Bleeding gums and nose – Spleen engorged leading to low platelets and WCC Leuconychia – Low albumin Spider naevi – Raised oestrogens Gynaecomastia – Raised oestrogens Loss of body hair – Raised oestrogens Ascites – Portal hypertension Splenomegaly – Portal hypertension Oesophageal varices – Portal hypertension Caput medusae – Portal hypertension Hepatomegaly or small liver – Damage to the liver parenchyma Palmar erythema – Pathogenesis unknown Clubbing – Pathogenesis unknown Fetor hepaticus – Portal hypertension allows some chemicals to reach the lungs directly |
|
|
Which clotting factors may be affected by liver failure? |
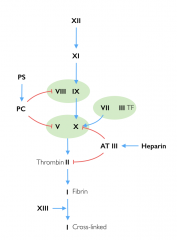
II, VII, IX, X |
|
|
How is the diagnosis of cirrhosis confirmed? |
Liver biopsy confirming the presence of nodules of regenerating hepatocytes surrounded by broad bands of fibrous tissues. |
|
|
A man with a known history of alcohol excess presents to the hospital with a one day history of confusion and agitation. On further questioning, he explains that he has decided to quit drinking 4 days ago. What is the likely diagnosis and what is the mechanism? |
Delirium tremens Alcohol excess (usually) ⟹ GABA receptors are potentiated ⟹ GABA receptor down-regulationAlcohol stopped abruptly ⟹ GABA activity ➘➘ ⟹ “Overactivity” |
|
|
Name 3 symptoms of delirium tremens |
Agitation Aggression Confusion Hallucinations Palpitations (arrhythmias) |
|
|
Name one context in which delirium tremens is particularly prevalent |
Alcoholic admitted to hospital as it may not receive his dose of alcohol |
|
|
Name 3 physical signs of delirium tremens |
Irregular HR Shaking Shivering Sweating |
|
|
What two things may you prescribe to a patient in alcohol withdrawal? |
Benzodiazepines Thiamine (B1), B6 and B12 |