![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
164 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
Order of Ischemia |
Ischemia-RWMA-ECG Changes- Painrep |
|
|
|
Repeat echoes are done on patients suffering from CAD T or F |
True |
|
|
|
Stress echo is valuable in predicting what two things? |
Myocardial viability (prognosis) Detection of CAD |
|
|
|
Role of echo in CAD |
Diagnose CAD Detect MI RWMA after reperfusion therapy Post MI function Assess myocardial viability |
|
|
|
What is the most commonly encountered problem in adult cardiology in the US? |
CAD |
|
|
|
Define ischemia |
Inadequate blood supply and oxygen to myocardium |
|
|
|
FUNCTIONAL outcome of CAD |
Systolic function (wall motion and systolic thickening) Diastolic function |
|
|
|
What happens with no blockage of coronary artery? |
No CAD, refer pt back to doctor |
|
|
|
What happens with a small blockage of a coronary artery? |
Pt referred back for medical therapy |
|
|
|
What happens with one or two blockages in coronary artery? |
Continue with angioplasty- gold standard |
|
|
|
What happens with multiple blockages of coronary artery? |
Candidate for CABG |
|
|
|
Define PTCA Explain procedure of PTCA |
Percutaneous Transluminal Coronary Angioplasty
Thin wire across the area of the blockage, balloon is inflated one or more times to open artery, stent may be deployed |
|
|
|
What is another name for prinzmetals angina |
Variant angina |
|
|
|
Meds used in CAD |
Nitrates BB Calcium antagonist Digitalis glycosides |
|
|
|
Name kinds of Nitrates used to treat CAD |
Isordil Isosorbide dinitrate Nitroglycerin Cardolite Nitrobid |
|
|
|
What do nitrates do? |
Vasodilator Reduces RV and LV preload Decreases cardiac work Lowers o2 requirements |
|
|
|
What is the first drug of choice for treating acute anginal attacks? |
Nitrates (NTG most common) |
|
|
|
Names for Beta Blockers? |
Inderal Corgard Lopressor Tenormin Atenolol |
|
|
|
What do beta blockers do? |
Reduce HR Reduces contractility Reduces systemic BP |
|
|
|
What are names of calcium channel blockers (calcium antagonists)? |
Calan Cardizem Diltiazem Nifedipine Procardia Verapamil |
|
|
|
How do calcium channel blockers work? |
Potent arterial vasodilators Decreases contractility Decreases HR Potent coronary vasodilators Increases coronary flow |
|
|
|
N+B=C |
Vasodilators+ decreases HR and contractility= potent vasodilator and decrease HR/ Contractility |
|
|
|
What are other names for digitalis? |
Digoxin Lanoxin |
|
|
|
What are other names for digitalis? |
Digoxin Lanoxin |
|
|
|
What do digitalis glycosides do? |
Increase resistance Increase contractility Increase HR promotes fluid elimination from tissues Used to treat some arrhythmias |
|
|
|
Names for ACE inhibitors |
Lasix Furosemide |
|
|
|
What do ACE inhibitors do? |
Prevents constriction of blood vessels Decreases after load Increases contractility |
|
|
|
Define stroke volume What is the formula |
Amount of blood ejected from the ventricle with each beat SV (cc)=LVOT D^2(cm) x .785 xLVOT TVI (Cm) |
|
|
|
Define cardiac output What is the formula |
Volume of blood ejected per minute CO (L/min)= SV x HR |
|
|
|
Define cardiac output What is the formula |
Volume of blood ejected per minute CO (L/min)= SV x HR |
|
|
|
What is cardiac index What is the formula |
Cardiac output per square meter of BSA CI (L/min/m^2) = CO/BSA |
|
|
|
Define cardiac output What is the formula |
Volume of blood ejected per minute CO (L/min)= SV x HR |
|
|
|
Describe athrectomy |
Catheter with grinding device Plaque ground into small bits and float away |
|
|
|
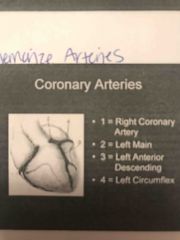
Know coronary arteries |
|
|
|
|
Which artery nourishes the most volume of the LV? |
LAD |
|
|
|
The dominant artery (PDA) supplies the _____________ wall of the LV |
INFEROLATERAL |
|
|
|
What prevent of LV is nourished by the LAD? |
50% |
|
|
|
What percent of the LV is nourished by the RCA? |
25% |
|
|
|
What percent of the LV is nourished by the LCX? |
25% |
|
|
|
What are the branches of the Lefr Main? |
LAD (50%) LCX (25%) |
|
|
|
Order of wall motion scoring: |
1- norm 2-hypo 3-akinetic 4-dys 5-aneueysmal |
|
|
|
Normal WMSI means what? |
Systolic contraction and wall thickening >50% |
|
|
|
Hypokinetic WMSI means what? |
Reduced systolic wall thinking <40% |
|
|
|
Akinetic WMSI means what? |
Diastolic wall thickness is thin and thinking in <10% or none |
|
|
|
Aneurysmal WMSI means what? |
Constantly deformed segment through entire cycle |
|
|
|
Coronary arteries primarily fill in______________ |
Diastole |
|
|
|
WMSI equals ? |
Sum of scores/ # of segments visualized. No less than 1 and anything greater than 2 is at risk of CHF, Arrythmias, death |
|
|
|
Course of Ischemia (time frame) |
Ischemia 00s-RWMA 20S- ECG 30S-Pain40s |
|
|
|
WHY STRESS echo with CAD |
A decrease in wall thickening=immediate MI non-inv Inexpensive Imm results God idea for treatment/ prognosis |
|
|
|
What characterizes significant stenosis? |
>50% lumen >70% lumen can cause disabling angina |
|
|
|
Describe PTCA |
Balloon catheter inserted through coronary artery Passed through lesion and expanded Relieves angina and reduce RWMA from exercise |
|
|
|
What is CABG |
Creates other pathways as healthy vessels called collaterals |
|
|
|
What is the purpose of stress test? |
TO INDUCE ISCHEMIA |
|
|
|
What is the goal of stress test? |
To have patient REACH TARGET HR |
|
|
|
Name the types of stress testing |
SEKG TMSE SMSE DSE |
|
|
|
Procedure for SEKG |
12 lead EKG Resting EGK and BP Exeecised
|
|
|
|
_______ and _______ coronary arteries feed the free wall |
LAD, LCX |
|
|
|
End points of SEGK |
Targt HR EKG changes develop Abnormal BP response Shows symptoms |
|
|
|
Describe TMSE |
12 lead EKG Baseline echo Impost echo _______________ Final rest echo (not everywhere rakes these images) |
|
|
|
Name the indications for TMSE |
CAD- known/ suspected CP, SOB Risky patients before surgery Abnormal ECG To identify viable stunned and hibernation |
|
|
|
When NOT to do a TMSE |
Acute MI (2 days) Unstable CP Vent. Arrythmias AS>50mmHg Acute PE PERICARDITIS PREGNANCY |
|
|
|
Protocol for TMSE |
12Lead EKG Resting echo Bruce protocol Impost echo Final test echo |
|
|
|
What is BRUCE protocol |
3 minute stages until may HR (85%) reached Starts at 1.7 mph at 10% incline |
|
|
|
What is modified BRUCE protocol |
Used for elderly/sedentary |
First 2 stages at 1.7 mph and 0% grade |
|
|
Know naughton protocol for TMSE |
2 minute stages increase by 3.5% each time. Used for people who are elderly/ sedentary and can still exercise |
|
|
|
Stop stressing if: |
Target HR reached EGK changes show ST depression Abnormal BP Showing significant symptoms |
|
|
|
Advantages of TMSE Disadvantages of TMSE |
Non invasive High total work load
Imaging after exercise RWMA could be missed |
|
|
|
_______ and _______ arteries feed the septum |
LAD, RCA |
|
|
|
When is DSE used? |
Used for elderly or for patients who have skeletal problems or past surgeries that make it difficult to exercise |
|
|
|
DSE consists of: |
Medication via IV infusion that mimics physical exercise. Performed for the same reasons as TMSE |
|
|
|
Whay happens Pre DSE |
12 lead resting ECK IV started Resting echo |
|
|
|
During DSE after set up: |
Infusion begins 5,10,20,30,40 MCG/KG/MIN 3 minute stages and 5 total stages ATROPINE may be added |
|
|
|
Echo images for DSE: |
Resting echo Low dose (1 or 2) echo Peak dose (5 or sooner if HR reached) echo Recoceey final echo |
|
|
|
Side effects of Dobutamine |
Tingling in head, scalp, face Tremors, nauseous |
|
|
|
Why do DSE? (Two big reasons) |
Determine if one will benefit from revasvularization Determine Stunned, hinernating, or infected heart muscle |
|
|
|
___________ myocardium is hypo or akinetic at rest and improved with low doses of Dobutamine |
Hinernating |
|
|
|
___________ myocardium can have a bi-phasic response to dobitamine- can get better with low doses and worse with high doses |
Hibernating |
|
|
|
What word is mostly related to "stunned" myocardium |
REPERFUSION- after the act of opening up blocked arteries |
|
|
|
How do you define coronary artery dominance? |
The origin of the PDA |
|
|
|
SBSE have the same indications as TMSE and can asses patients with AS or MS |
Blank |
|
|
|
Protocol for SBSE |
Rest images Exercised at 25 watts and 60 RPM Icreases every 2 minutes by 25watts Peak images Impost images Final rest images |
|
|
|
Quad screen for SBSE |
REST PEAK IMPOST FINAL |
|
|
|
Quad screen for TMSE |
REST IMPOST A4C, A2C, A3C/ PLAX, PSAX MID |
|
|
|
Advantage is SBSE Disadvantages of SBSE |
Able to image at exact peak stress
Problem of workload- pt finds it hard to bike supine and have inadequate level of stress |
|
|
|
Creatine kinase (CK) is a later marker in cardiac cell damage. Elevates in ___ to___ hours Peaks ___ to ___ house Falls ____ to ____ |
3-12 12-24 1-3 |
|
|
|
Negative stress echo means______ |
-tested negative for CAD -Normal wall motion and -hyperdynamic with stress |
|
|
|
Positive stress test means _________ |
Wall motion became either -hypo -akinetic -dyskinetic -Increase in size and shape of LV -Decrease in EF% |
|
|
|
False positive stress test means__________ |
Positive SEKG but negative stress test |
|
|
|
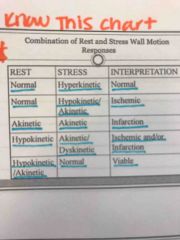
What is a normal response to stress of the myocardium? |
Decrease in ESV and EDV |
|
|
|
Interpreting stress echoes **know this chart |
|
|
|
|
What is an abnormal response to stressing the myocardium? |
Failure of ESV to decrease Increase in volume can indicate severe and extensive multi-velles disease |
|
|
|
The LV should always increase in size when stressing the myocardium T or F? |
False- should ALWAYS decrease |
|
|
|
False negative |
Not reaching target HR collaterals from single vessel disease present |
|
|
|
Which of these are reversible: ischemia, stunned, hibernating? |
All are reversible and viable |
|
|
|
Ischemia will show wall motion abnormalities of what kind? |
Hypokinetic or akinetic Wall motion will return to normal at rest |
|
|
|
Stunned myocardium is viable and occurs after opening up previously blocked arteries T or F? |
True |
|
|
|
What kind of wall motion abnormalities is irreversible? |
Necrtoic tissue caused by infarction |
|
|
|
What to expect for wall motion with an active MI? |
Akinetic with normal wall thickness
Opposing walls may be hyperkinetic |
|
|
|
Name some other modalities to assess ischemia |
Doppler stress echo Intravascular US Contrast Agents Ultrafast CT Angiography **gold standard Nice med uses thallium as a tag PET Positron Emission Tomography |
|
|
|
This term means disease of the intima that gets thick with fatty deposits and fibrous tissue |
Atherosclerosis |
|
|
|
LCX gives rise to the PDA ___% Of the time |
10% |
|
|
|
With atherosclerosis the intima gets _______ and the lumen gets_________ |
Smaller, bigger |
|
|
|
Acute lesions due to atherosclerosis can cause ruptures and thrombus formations. These are unpredictable and can lead to: |
Unstable anyone Acute MI Sudden death |
|
|
|
How narrowed does a coronary artery have to be before a patient experiences symptoms with exercise? |
75% |
|
|
|
How narrowed does a coronary artery have to be u til a patient experiences symptoms at rest? |
90% (critical lesions) |
|
|
|
3 vessel disease can happen and this is when all the vessels are narrowed at the same time T or F |
True |
|
|
|
How the heart works is a better indicator than how occluded an artery is for prognosis of CAD T or F |
True |
|
|
|
Arteriosclerosis consists of: |
Hardening of art walls Loss of elasticity of art walls Thickening of arterial walls |
|
|
|
ASHD (Arteriosclerotic heart disease) is defined as: |
Thickening and hardening of Walls of the coronary arteries leads to narrowing of the coronary lumen |
|
|
|
When the RCA supplies the PDA it is ________ dominance |
Right |
|
|
|
When the LCX gives rise to the PDA it is ______ dominance |
Left |
|
|
|
Both RCA and LCX gives rise to the PDA____% Of the time |
20% co dominant |
|
|
|
Troponin is an early marker of cardiac cell damage. Elevates ____ to ____ hours after an MI. Peaks within ____ to ____ hours. Falls >____ days |
3-6 10-24 7 |
|
|
|
Aspartate transaminase (AST) Elevates in ____ to ____ house. Peaks ___ to ____ hours Falls ___ to ___ days |
8-12 24-48 3-5 |
|
|
|
Aspartate transaminase (AST) Elevates in ____ to ____ house. Peaks ___ to ____ hours Falls ___ to ___ days |
8-12 24-48 3-5 |
|
|
|
Lactic (Lactate) Dehydrogenase (LDH) gives a longer period of time is cardiac enzymes were missed. Elevates in ___ to ___ hours Peaks in ___ to ___ hours Falls ___ to ___ days |
24-48 48-72 7-14 |
|
|
|
What happens during a follow up for an MI |
Look for stunned myocardium Observe WMA Observe other MI related complications short and long term |
|
|
|
Describe each week after an MI: Week 1: Week 2: Week 3-4: |
Week 1: inflammation stage increase in WBC Week 2: clean up stage cleans out tissue debris Week 3-4: healing phase, scarring forms |
|
|
|
This disease consists of areas of akinesis and thinned myocardium. Also RV could be functioning and looking normal. -MR may be present -Creates elevated PA pressures |
Ischemia Heart Disease |
|
|
|
Characteristics of DCM |
Imore gloabal RWMA Both LV and RV are DILATED Hypokinetic Moderate to severe TR Elevated PA pressures |
|
|
|
Lifestyle changes for CAD |
SMOKING HTN HIGH LDL DIABETES OBESITY SEDENRARY STRESS |
|
|
|
Lifestyle changes for CAD |
SMOKING HTN HIGH LDL DIABETES OBESITY SEDENRARY STRESS |
|
|
|
Things you cannot control for CAD |
AGE FAMILY HISTORY MALE POST-Menapausal |
|
|
|
Lifestyle changes for CAD |
SMOKING HTN HIGH LDL DIABETES OBESITY SEDENRARY STRESS |
|
|
|
Things you cannot control for CAD |
AGE FAMILY HISTORY MALE POST-Menapausal |
|
|
|
What are the warning signs of a heart attack? |
CP PAIN IN UPPER BODY (Arms neck jaw back stomach) SOB Nausea Anxiety Lightheadedness |
|
|
|
Fact: among people with coronary atherosclerosis who suffer and acute MI 50% will die within one hour |
Blank |
|
|
|
Fact: among people with coronary atherosclerosis who suffer and acute MI 50% will die within one hour |
Blank |
|
|
|
Fact: of those who survive and have a diagnosis of MI 50% will have uncomplicated Hosp. Stay and 50% will experience complications |
Blank |
|
|
|
When an infarct expands the volume does not increase but the region stretches and thins causing an outward bulging of the area during SYSTOLE known as dyskinesis |
Not a good prognosis |
|
|
|
A Ture aneurysm is lined by _______ and has no ______ |
Myocardium, neck |
|
|
|
True aneurysms are only found in __________ MI |
Transmural |
|
|
|
A pseudoaneurysm is contained by the ___________due to a ventricular rupture. Has a ______ |
Pericardium, neck |
|
|
|
A pseudoaneurysm is contained by the ___________due to a ventricular rupture. Has a ______ |
Pericardium, neck |
|
|
|
Pseudoaneurysm S see only found in ___________ MI |
Transmural |
|
|
|
Cardiac ruptures are very likely with pseudoaneurysms and tend to occur within the first ________ |
Week |
|
|
|
This is a common response to having an acute MI: |
Pericaardial effusion |
|
|
|
What is the biggest indicator for healing after an MI? |
How good the LV is functioning |
|
|
|
EKG consist of ______ wires and ______ leads |
10,12 |
|
|
|
Papillary muscle rupture creates rocking or flail at valve site **80% posteromedial **20% anterolateral |

|
|
|
|
What are the 6 chest leada? |
V1,V2,V3,V4,V5,V6 |
|
|
|
What is another name for the bipolar leads on an EKG? |
Limb leads |
|
|
|
What are the three bipolar leads? |
1,2,3 |
|
|
|
What is another name for unipolar leads on an EKG? |
Augmented limb leads (hence the a) |
|
|
|
What are the three augmented or unipolar limb leads? |
aVR, aVL, aVF |
|
|
|
Order of EKG wave form: |
P wave PR QRS ST T T TO P |
|
|
|
Name three types of pseudoaneurysm |
Free wall Ventricular septal Papillary muscle |
|
|
|
Interpreting EGK: ST segment depression and any lead but a VR means
ISCHEMIA SUBENDOCARDIAL INFARCT |
BLANK |
|
|
|
Interperetinf EKG: an ST segment elevation any lead but aVR indicates
ACUTE MI PERICARDITIS TAMPONADE CARDIAC CONTUSION |
BLANK |
|
|
|
Interpreting EKG: significant Q waves any lead but aVR represents an old MI or an MI. **1mm wide (.04 sec) and at least 1/3 the height of QRS |
**know stars |
|
|
|
Normal finding on EKG: -T wave in V2-V6 upright Abnormal finfing: -flattened T wave means ischemia -inberted T wave means ichemia
|
T wave: Upright= normal Flattened= ischemia Inverted=ischemia |
|
|
|
Anterior infarct will show on leads____ ______ |
V3, V4 |
|
|
|
Lateral infarct will show on leads ____ ____ _____ _____ |
V5, V6, 1, aVL |
|
|
|
Inferior infarct will show on leads ___ ___ ____ |
2, 3, aVF |
|
|
|
Septal infarct will appear on leads ___ ____ |
V1, V2 |
|
|
|
RV infarct will show on leads : |
V4R |
|
|
|
A free wall rupture causes pressure buildup causing cardiac tamponade (an irregular way of beating due to pressure) **85% of cases **look for effusion ** Only in transmural MI |
Know the stars** |
|
|
|
A ventricular septal rupture can lead to a shunt VSD - new loud harsh systolic murmur -bad prognosis -50% mortality |
Blank |
|
|
|
Papillary muscle rupture creates rocking or flail at valve site **80% posteromedial **20% anterolateral |
|
|
|
|
Clots form in areas where: |
Dilated areas Areas with WMA |
|
|
|
Define "smoke" |
"smoke" means spontaneous echo contrast and represents blood pooling and stagnation |
|
|
|
Types of thrombus: |
**Predunculated: finger like and protrudes into LV and moves around Mural: adheres to the ENDOcardium and creates areas that are dense and thickened Hyper eosinophilia: common in apex not related to MI |
|
|
|
** Dressler's syndrome is a syndrome that occurs post MI WEEKS TO MONTHS LATER. Symptoms include: |
Chest pain Low grade fever Friction rub PE |
|
|
|
Cariogenic shock consists of the loss of at least 40% of LV mass and may lead to death. People have abnormal CO |
Blank |
|