Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
101 Cards in this Set
- Front
- Back
|
What can myeloid stem cells differentiate into?
|
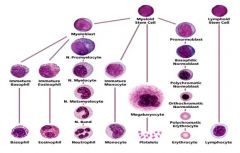
Basophils
Eosinophils Neutrophils Monocytes Platelets Erythrocytes |
|
|
What can myeloblasts differentiate into?
|
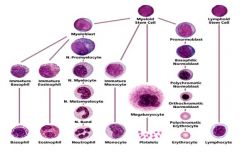
Basophils
Eosinophils Neutrophils |
|
|
What disease is associated with N. promyelocytes?
|
Severe congenital neutropenia
There's an arrest in the bone marrow maturation |
|
|
What are the properties of the neutrophil?
|
Common
Nucleus is 2-5 segments Light pink granules Diameter: 12-15 uM |
|
|
What are the properties of the monocyte?
|

Commonly observed
Horse-shoe shaped nucleus Diameter: 16-20 uM |
|
|
What are the properties of the eosinophil?
|

Rare
Bi-lobed nucleus Vibrant pink-orange granules Diameter: 12-17 uM |
|
|
What are the properties of the basophil?
|

Very rare
Bi-lobed nucleus Large blue-purple granules Diameter: 9-10 uM |
|
|
Where does neutrophil differentiation take place?
|
Bone marrow: proliferiation, maturation
Circulation: final differentiation |
|
|
How long does neutrophil maturation take?
|
14 days
|
|
|
How many of the neutrophils are in the proliferation phase?
|
25%
6-7 days while proliferating |
|
|
What are the proliferative neutrophils?
|
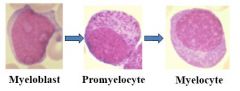
Myeloblasts
Promyelocyte Myelocyte Mitotic |
|
|
How many of the neutrophils are in the maturation phase?
|
65%
Total of 6-7 days maturing |
|
|
What are the maturing neutrophils?
|

Metmyelocyte
Bands Neutrophils |
|
|
What percentage of neutrophils are normally in the tissue? Circulation?
|
Tissue: 2%
Circulating: 10% |
|
|
What;s the NL for neutrophils?
|
1.5-8.0 E 9 cells/L
|
|
|
What's the definition of moderate neutropenia? Severe?
|
Moderate: .5-1.0 E9 cells/L
Severe: 0-.5 E9 cells/L The lower the neutrophil levels, the more severe the risk of infection. |
|
|
What are the normal levels of neutrophils for term infants? Infants? Kids?
|
Term infant: 3,000
Infant: 1,100 Kids, adolescent, adults: >1,500 |
|
|
What ethnic groups have lower absolute neutrophil counts?
|
African-americans.
They don't have symptoms, though! |
|
|
How do you calculate the absolute neutrophil count (ANC)?
|
ANC = (% bands + % segmented neutrophils) * total WBC
|
|
|
When should you have a clinical suspicion for neutropenia?
|
Acute, severe bacterial infection
History of recurrent/rare infections Prolonged or recurrent fevers Recurrent mouth ulcers, chronic gingivitis, cellulitis, perirectal abscesses Findings associated with malignancy, immunodeficiency or syndrome |
|
|
What is unique about the height and weight of patients with neutropenia?
|
Short stature compared to weight
|
|
|
Where are there often abnormal findings in a neutropenic patient?
|
Oral cavity!
|
|
|
What parts of the extremities are commonly compromised in patients with neutropenia?
|
Forearms
Thumbs |
|
|
What oral findings are characteristic of a patient with neutropenia?
|

|
|
|
What's usually the cause of neutropenia?
|
Infection (virus, normally)
Drug-induced Immune-based |
|
|
What patients are particularly vulnerable to neutropenia?
|
Neonates
They can exhaust their bone marrow/reserve neutrophils easily->bacterial sepsis |
|
|
What are the common mechanisms for drug-induced neutropenia?
|
Toxic
Immunologic Hypersensitivity |
|
|
What are some common drug classes that cause neutropenia?
|
Anticonvulsants
Antipsychotics Antibiotics: chlorampehicol, bactram |
|
|
What are the different types of immune-based acquired neutropenias?
|
Alloimmune neutropenia of infancy
Autoimmune neutropenia of infancy |
|
|
How does the alloimmune neutropenia of infancy occur?
|
Passive transfer of maternal IgG against fetal neutrophils
Once the antibodies are cleared, the patient gets better This can happen with the first pregnancy - a way to differentiate from Rh disease |
|
|
How does the autoimmune neutropenia of infancy occur?
|
Appears around 1 year
ANC of 200-300 is classic Treatment isn't really indicated; the reserve is still there. |
|
|
What are the different types of inherited neutropenias?
|
Primary disorders of myelopoiesis
Disorders of ribosomal function Disorders of granule sorting/trafficking Disorders of metabolism Neutropenia in disorders of immune fuction |
|
|
What is the most common kind of congenital neutropenia?
|
Severe congenital neutropenia
|
|
|
What is the presentation of severe congenital neutropenia?
|
Infant presents in the first year of life with recurrent/severe infections
|
|
|
What's required for a diagnosis of severe congenital neutropenia?
|
Three ANCs < 500
|
|
|
What mutations are associated with severe congenital neutropenia?
|
ELANE (autosomal dominant)
HAX1 (autosomal recessive) |
|
|
What's the treatment for severe congenital neutropenia?
|
G-CSF
Bone marrow transplant |
|
|
What diseases are more common in patients with severe congenital neutropenia?
|
AML
MDS |
|
|
What is cyclic neutropenia?
|
Cycles of neutropenia
|
|
|
How long are the cycles in cyclic neutropenia?
|
21 days
7-10 days of neutropenia |
|
|
What's the presentationof cyclic neutropenia?
|
Presents before 1
Recurrent fevers, malaise, apthous ulcers, bacterial infections |
|
|
What bacteria are especially pathogenic to people with cyclic neutropenia?
|
Clostridium septicum
|
|
|
How do you diagnose cyclic neutropenia?
|
You do CBCs 2-3 times/week for 6 weeks
|
|
|
What gene is mutated in cyclic neutropenia?
|
ELANE gene
|
|
|
What's the treatment for cyclic neutropenia?
|
G-CSF
Shortens the duration of the neutropenia NO RISK OF LEUKEMIA |
|
|
What is the definition of neutrophilia?
|
Abnormally high neutrophil counts
|
|
|
What's the cause of neutrophilia?
|
Acute shift from the marginating pool to the circulating pool
Chronic stimulation with excess cytokines increasing the proliferating pool |
|
|
What are some things that can cause neutrophils to shift to the circulating pool from the marginating pool?
|
Steroids
Exercise Epinephrine Hypoxia Seizures |
|
|
What are somethings that can cause chronic proliferation of neutrophils?
|
Infections
G-CSF Pregnancy Trisomy 21 Recovery from chemo Myeloproliferative disorders |
|
|
What are the stages of neutrophil killing?
|
1. Mobilization
2. Chemotaxis 3. Recognition/opsinization 4.Ingestion 5. Degranulation 6. Peroxidation 7. Killing and digestion 8. Net formation |
|
|
What is myelokathexis?
|
Apoptosis and retention of neutrophils in the bone marrow
|
|
|
What gene is mutated in myelokathexis?
|
CXCR4 chemokine receptor
|
|
|
What are the clinical characteristics of myelokathexis?
|
WHIM!
W: warts H: hypergammaglobulinemia I: infections M: myelokathexis |
|
|
What's the treatmnet for myelokathexis?
|
G-CSF
CXCR4 antagonist |
|
|
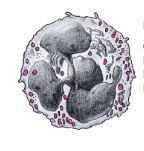
What is the apperance of neutrophils in WHIM syndrome?
|
Lots of segmentation of the neutrophils in the bone marrow.
|
|
|
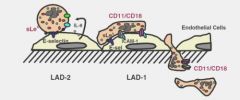
What are the steps of neutrophil migration into tissues?
|
|
|
|
What molecules are involved in neutrophil rolling?
|
Selectins
|
|
|
What molecules are involved in adhesion of the neutrophils to the endothelium?
|
CD11/CD18
|
|
|
What are the findings in leukocyte adhesion deficiency?
|
Neutrophilia
Infections Absence of pus formation Impaired wound healing Delayed umbilical cord separation (LAD1) |
|
|
What is the classic oral finding in LAD?
|
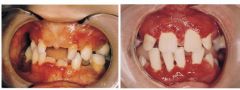
Peridonitis
|
|
|
What defect is present in LAD1? What process is inhibited?
|
B2 integrin CD18
Adhesion |
|
|
What's the treatment for LAD1?
|
Bone marrow transplant
|
|
|
What molecules are mutated in LAD1? What process is inhibited?
|
Selectins
Rolling; can't be tethered to the tissue |
|
|
What are the findings in LAD2?
|
Neurologic defects
Craniofacial anamolies Rare erythrocyte phenotype |
|
|
What's the treatment for LAD2?
|
Very little we can do for them.
|
|
|
What gene is mutated in LAD3? What process is inhibited?
|
Kindlin
Integrin activation |
|
|
What are the findings in LAD3?
|
Neutrophil AND bleeding problems.
|
|
|
What is Chediak higashi syndrome?
|
Autosomal recessive disorder
|
|
|
What are the findings in Chediak higashi syndrome?
|
Immunodeficiency
Partial oculo-cutaneous albinism Bleeding diathesis Progressive neurologic deterioration Oddly colored hair |
|
|
What process are people with Chediak Higashi syndrome unable to perform?
|
Granule trafficking in neutrophils
You see giant neutrophils! |
|
|
What gene is mutated in Chediak higashi syndrome?
|
CHS1/LYST gene
Responsible for lysosomal trafficking |
|
|
What are people with chediak higshi syndrome vulnerable to?
|
Hemophagocytic lymphohistiocytosis: can't turn off phagocytois
Hepatomegaly, splenomegaly |
|
|
What's the treatment for Chediak higashi syndrome?
|
Antibiotics
G-CSF Bone marrow treatment (cures hematologic, immunodeficiency problems, doesn't affect albinism/neurologic features) |
|
|
What are the different types of neutrophil granules?
|
Primary: neutral proteases, myeloperoxidase
Secondary: lactoferrin Tertiary: gelatinase Secretory: alkaline phosphatase |
|
|
What are the findings in myeloperoxidase deficiency?
|
Largely asymptomatic
Only see disease in people with diabetes |
|
|
What is the action of myeloperoxidase?
|
Forms bleach from H2O2 and chloride
|
|
|
What organism is particularly targeted by the formation of HOCl in the body?
|
Candida
|
|
|
How does acquired MPO deficiency happen?
|
You get a disruption of the bone marrow that causes an induced mutation
|
|
|
What is the treatment for MPO?
|
Very little for the disease itself
Aggressively manage the fungal diseases Control the glucose tightly if there's DM |
|
|
What occurs in chronic granulomatous disease?
|
Mutation in NADPH oxidase-->no superoxide
Can't destroy catalase-positive microbes |
|
|
What kinds of infections are people with CGD vulnerable to?
|

S. aureus
Aspergillus |
|
|
Where do you get infections in CGD?
|
Lungs
Skin Lymph nodes LIVER |
|
|
What's commonly mutated in NADPH in CGD?
|
gp91phox: 65%; X-linked
p47phox: 25%; autosomal recessive |
|
|
How do you go about diagnosing CG?
|
Rhodamine dye test: dye is taken up by phagocytes-->oxidized; fluoresence
Nitroblue tetrazolium test: changing the color of a dye when superoxide is produced |
|
|
What's the treatment for CGD?
|
Antimicrobial prophylaxis: bactram
Immune modulation: interferon gamma Aggressive treatment of infections Bone marrow transplant is the only cure |
|
|
What process needs to be intact for net formation to occur? What disease states cannot perform this?
|
Hydrogen peroxide production
CGD MPO |
|
|
What are the stages of monocyte differentiation?
|
Proliferation
Maturation SHorter tissue phase They then differentiate into macrophages |
|
|
What's the usual monocyte count?
|
300/uL
|
|
|
How long does it take monocytes to arrive at the scene?
|
12 hours
|
|
|
What are causes of a low monocyte count?
|
Stress
Endotoxemia Glucocorticoids |
|
|
What are causes if high monocyte counts?
|
Bone marrow disease
Infection Inflammatory disease |
|
|
What are the stages of eosinophil naturation?
|
Proliferation (9 days)
Maturation Intravascular |
|
|
What is the precursor to eosinophils?
|
Myeocytes
|
|
|
What are some causes of eosinopenia?
|
Infection
Corticosteroids Prostaglandins Epinephrine No additional risks from having this |
|
|
What is eosinophilia? What are causes?
|
>500/ uL
Causes: Neoplasms Allergies Asthma Collagen vascular diseases |
|
|
What are the characteristics of idiopathic hypereosinophilic syndrome?
|
>1500 cells/uL for 6 months
Happens in people who are 20-50 Lots of organ dysfunction |
|
|
What is the cause of pathology in idiopathic hypereosinophilic syndrome?
|
Large scale eosinophil degranulation and release of major basic protein into the tissues
You can also get an eosinophilic leukemia |
|
|
How long do basophils live in the tissues?
|
A long time!
Up to days |
|
|
What are causes of low basophil counts?
|
Hypersensitivity
Glucocorticoids |
|
|
What's the role of the basophil?
|
Unknown.
|
|
|
What causes a high basophil count?
|
Allergies
Infections Endocrinopathies Myeloproliferative disorders Systemic mastocytosis |