![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
84 Cards in this Set
- Front
- Back
|
FETAL PLACENTAL PART IS FROM WHAT? |
Frondusum |
|
|
MATERNAL PLACENTAL PART IS FROM WHAT? |
Chorionic plate |
|
|
WHAT IS THE SECOND SURFACE OF THE MATERNAL PORTION OF PLACENTA? |
Basal plate |
|
|
WHERE DOES THE BASAL PLATE LIE? |
At junction of myometrium and substance of placenta |
|
|
WHEN CAN PLACENTA BE IDENTIFIED? |
As early as 8 weeks |
|
|
BETWEEN 8 AND 20 WEEKS, HOW SHOULD PLACENTA LOOK ON US? |
Homogenous mid level gray appearance, easily recognized, with smooth borders |
|
|
AFTER 20 WEEKS GESTATION, WHAT CHANGES MIGHT TAKE PLACE WITH THE PLACENTA SONOGRAPHICALLY? |
Intraplacental sonolucencies and placental calcification may begin to appear |
|
|
THICKNESS VARIES WITH GA, BUT USUALLY MEASURES WHAT? |
2 to 3 cm in fetuses greater than 23 weeks |
|
|
NORMAL PLACENTA RARELY EXCEEDS WHAT MEASUREMENT? |
4 cm |
|
|
HOW IS THE PLACENTA CLASSIFIED ACCORDING TO SONOGRAPHIC APPEARANCE? |
Grade0 Grade1 Grade2 Grade3 |
|
|
GRADE 0 PLACENTA |
representnormal placenta throughout the pregnancy, smooth border, homogeneous with lowlevel echoes |
|
|
GRADE 1 PLACENTA |
subtleindentation, with few scattered calcification, this also considered as normalplacenta up to 34 weeks of development. |
|
|
GRADE 2 PLACENTA |
exhibitsmedium indentation, and scattered coma tail like calcification, also can benormal finding after 36 weeks of development |
|
|
GRADE 3 PLACENTA |
deepindentation that extend between basal layer and chorionic plate dividing placenta into segments, placenta will appearhyper echoic with more calcification that may cause acoustic shadowing, alsocab be normal finding after week 38 of development |
|
|
HOW DO WE SCAN THE PLACENTA? |
TA or TV |
|
|
HOW DO WE SCAN PLACENTA TA? |
Longitudinallyfrom side to sidE (right to left) Tranverselyfrom inferior to superior |
|
|
WHAT SHOULD YOU DO WITH THE INSERTION OF CORD INTO PLACENTA? |
Visualize Describeas mid placental, marginal, or velamentous |
|
|
WHAT IS MEANT BY: Inferioredge documented to evaluate its relationship to internal cervical os. |
How far the placenta is from the internal os |
|
|
HOW DOES FULL BLADDER AFFECT PLACENTA? |
Placenta will be pushed down and represent false location cervix is falsely elongated normally implantedplacenta may appear to be covering internal cervical os maygive false impression of previa |
|
|
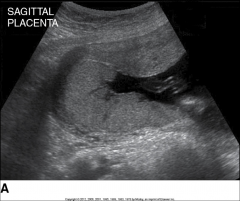
Sagittalview of the uterus reveals a posterior fundal placenta. |
|

|
Transverse view of the uterusdemonstrates a right side wall placenta that extends along the anterior wall ofthe uterus. |
|

|
Transabdominalimage of placenta previa. |
|
|
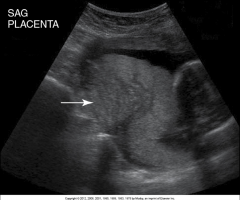
BraxtonHicks. (False contractions) Uterine contraction (arrow) isseen distorting the placenta. |
|
|
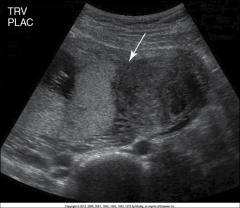
Transverse view of the uterusreveals a hypoechoicuterine myoma (arrow).Theleft side wall placenta is implanted on the myoma. |
|
|
Theplacenta is implanted away from the os. Complete previa |
|
|
WHAT ARE CAUSES OF PLACENTOMEGALY? |
Maternaldiabetes Maternalanemia α-Thalassemia Rhsensitivity Fetomaternalhemorrhage Chronicintrauterine infections Twin-twintransfusion syndrome Congenitalneoplasms Fetalmalformations |
|
|
ALPHA THALESSEMIA IS A TYPE OF WHAT? |
Anemia aka Meditteranean anema |
|
|
WHAT CARE CAUSES FOR SMALL PLACENTA? |
Intrauterine growth restriction Intrauterine infection Aneuploidy |
|
|
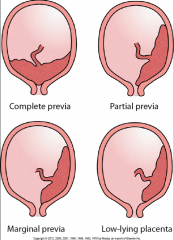
WHAT IS PLACENTA PREVIA? |
Implantationof placenta over internal cervical os |
|
|
NORMALLY, WHERE DOES THE PLACENTA IMPLANT? |
In body or fundus of uterus |
|
|
WHAT DOES THE RISK OF PLACENTA PREVIA INCREASE WITH? |
History of cesarean delivery |
|
|
WHAT DO YOU CALL IT WHEN THE INTERNAL OS IS COMPLETELY COVERED BY PLACENTA TISSUE? |
Complete previa
|
|
|
WHAT DO YOU CALL IT WHEN THE INTERNAL OS IS PARTIAL COVERED BY PLACENTA TISSUE BUT PLACENTA IS STILL TOUCHING THE INTERNAL OS? |
Partial previa |
|
|
WHAT DO YOU CALL IT WHEN THE INTERNAL OS IS NOT COVERED BY PALCENTA TISSUE, BUT ITS EDGE COMES TO THE MARINE OF THE OS? |
Marginal previa |
|
|
WHAT DO YOU CALL IT WHEN THE PLACENTA TISSUE IMPLEMENTED IN THE LOWER UTERIN SEGMENT, AND DOES NOT REACH THE INTERNAL OS, AND IS ASSOCIATED W/ NO SYMTPOMS? |
Low lying |
|
|
placenta previas |
|
|
WHAT ARE CAUSES AND RISK FACTORS OF PLACENTA PREVIA? |
Advancedmaternal age Smoking Cocaineabuse Priorplacental previa Multiparity Priorcesarean section Uterinesurgery |
|
|
WHAT ARE THE CONSEQUENCES OR COMPLICATIONS OF PLACENTA PREVIA? |
pretermdelivery maternal hemorrhage increased risk of placental invasion increased risk of postpartum hemorrhage IUGR |
|
|
WHAT IS THE CLINICAL PRESENTATION OF PLACENTA PREVIA? |
may present with painless, bright red vaginal bleeding in second/thirdtrimester |
|
|
MOST COMMON CAUSE OF 2ND AND 3RD TRIMESTER PAINLESS VAGINAL BLEEDING IS WHAT? |
Placenta previa |
|
|
HOW DO WE ID PLACENTA PREVIA IN TA? |
sonographerneeds to examine the location of the placenta in relation to the lower uterinesegment (carefully interpreting a lowlying placenta covering internal Os due to over distended bladder) |
|
|
HOW DO WE ID PLACENTA PREVIA IN TV? |
provepresence of placenta previa, ifthe edge of the placenta covers the internal Os more than 15mm (SINCE FROM THE BEGINNING OF PREGNANCY), it will probablynot resolve |
|
|
WHAT IS THE MOST ACCURATE METHOD IN IDENTIFYING PLACENTA PREVIA? |
Trans-labial |
|
|
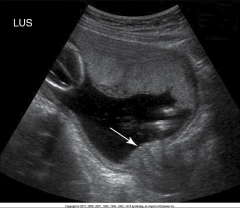
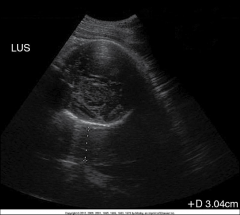
Alower uterine segment (LUS) in the longitudinal plane shows the placentaltissue (30 mm) lying between the maternal sacrum and the fetal head. This womanhad a complete placenta previa“Normallythe distance should be no more than 1.5cm” Baby is trying to engage head for delivery but this is not going to happen so there is going to be a lot of bleeding |
|
|
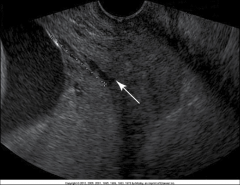
Completeprevia. Transvaginalimage of cervix reveals a posterior placenta covering ICO (arrow) andextending 29.5 mm anteriorly. This complete previapersisted until delivery |
|
|
WHAT IS PLACENTAL INVASION? |
Abnormalpenetrationof placental tissue beyondendometrial liningof uterus |
|
|
WHAT ARE THE THREE DIFF TYPES OF PLACENTAL INVASION? |
Placenta Accretia Placenta Increta Placenta Percreta |
|
|
PLACENTA ACCRETA |
Chorionic villi attach to myometrium without muscular invasion can be managed depending on how lucky you are |
|
|
PLACENTA INCRETA |
further extension of the chorionic villi into the myometrium morbidity increases with this |
|
|
PLACENTA PERCRETA |
penetration of the chorionic villi through the uterus morbidity increases with this |
|
|
WHAT IS PLACENTA INCREATE A RESULT OF ? |
Underdeveloped decidualization of our endometrium |
|
|
PLACENTA ACCRETA INCREASES IN PTs W/ WHAT? |
Previous cesarean scar "permits trophoblastic invasion" |
|
|
True of False: WE ARE UNABLE TO ID PLACENTA INVASION SONOGRAPHICALLY. |
True |
|
|
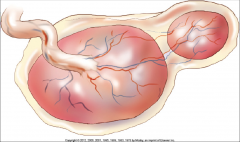
WHAT IS A SUCCENTURIATE PLACENTA? |
Presence of one or more accessorylobes connected to body of placenta by placental vessels |
|
|
IN WHAT PERCENTAGE DOES SUCCENTURIATE PLACENTA OCCUR IN PREGNANCIES? |
3-6% |
|
|
Asuccenturiateplacenta is the presence of one or more accessory lobes connected to the bodyof the placenta by blood vessels |
|

|
Transverseimage of the uterus reveals a left side wall placenta. Vessels (arrow) canbe seen connecting the accessory lobe, which is anterior |
|
|
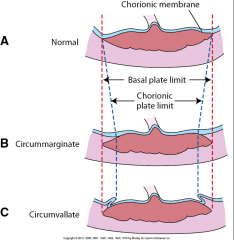
WHAT IS A CIRCUMVALLATE/CIRCUMMARGINATE PLACENTA? |
attachment of placental membranes to fetal surface of placenta rather than to underlying villous placental margin |
|
|
WHAT DOES CIRCUMVALLATE/CIRCUMMARGINATE RESULT FROM? |
Placental villi around borderof placent not covered by chorionic plate |
|
|
WHAT IS CIRCUMVALLIATE/CIRMMARGINATE ASSOCIATED WITH? |
PROM Preterm labor IUGR Placental abruption |
|
|
Comparisonof extrachorialplacentas with a normal placenta (A). Thetransition of membranous to villous chorion isat the placental edge. B, Circummarginateplacenta. The transition of membranous to villous chorionoccurs central to the edge of the placenta, but the chorionic surface remainssmooth. C, Circumvallate placenta. Thechorionic membrane is folding |
|
|
BLEEDING FROM THE PLACENTA FROM ANY CAUSE IS AKA...? |
Placental hemorrhage |
|
|
WHERE WOULD PLACENTAL HEMORRHAGE TAKE PLACE? |
retroplacental, subchorionic, subamniotic, and intraplacental sites |
|
|
THE ECHOGENICITY OF THE PLACENTAL HEMORRHAGE DEPENDS ON WHAT? |
Ageo f the hemorrhage |
|
|
T or F: ACUTE BLEED IS SIMILAR TO ECHOGENICITY OF PLACENTA. |
True |
|
|
DOES SUBACUTE AND CHRONIC PLACENTAL BLEEDB ECOMES MORE HYPOECHOIC OR HYPERECHOIC? |
Hypoechoic |
|
|
WHAT REFERS TO SEPARATION OF NORMALLY IMPLANTED PLACENTA PRIOR TO TERM DELIVERY? |
Placental abruption |
|
|
PREMATURE PLACENTAL DETACHMENT IS ANOTHER WAY OF SAYING....? |
Placental abruption |
|
|
PLACENTAL ABRUPTION OCCURS IN HOW MANY PREGNANCIES? |
1 in 120 |
|
|
HYPERTENSION AND VASCULAR DISEASE ARE ASSOCIATED WITH WHAT...? |
Placental abruption |
|
|
WHERE DOES THE HEMATOMA TAKE PLACE IN PLACENTAL ABRUPTION? |
Between placenta and uterus |
|
|
PATIENT WILL HAVE NO VAGINAL BLEEDING IF THE BLOOD REMAINS WHERE? |
Retroplacental |
|
|
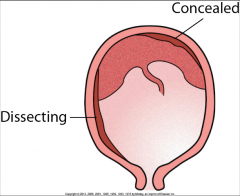
WHAT ARE TWO CLASSIFICATIONS OF PLACENTAL ABRUPTION? |
Placental Marginal |
|
|
Typesof placental abruption |
|
|
WHAT IS THE MOST COMMON TYPE OF ABRUPTION? |
Marginal aka subchorionic bleed |
|

|
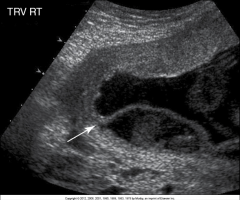
RETROPLACENTAL ABRUPTION Hypoechoichematoma is seen separating the placenta (arrow) fromthe uterine wall (curved arrow). |
|
|
MARGINAL ABRUPTION Subchorionicbleed can be seen arising from the edge of the placenta (arrow). |
|
|
FOCAL DISCRETE LESION CAUSED BY ISCHEMIC NECROSIS IS CALLED...? |
Placenta infarcts |
|
|
PLACENTA INFARCTS IS FOUND IN WHAT PERCENTAGE OF PREGNANCIES, USUALLY SMALL W/ NO CLINICAL SIGNIFICANCE |
25% |
|
|
UNDERLYING MATERNAL VASCULAR DISEASE IN CONECTION WITH INFARCTS IS THAT LARGE INFARCTS...? |
Large infarcts reflect them! |
|
|
WHAT ARE THE THREE STAGES THAT PLACENTA INFARCTS EVOLVE THRU? |
Acute, subacute, and chorionic stages |
|
|
IN ACUTE STAGE, THE MAJORITY OF PLACENTA INFARCTS ARE HYPER OR HYPOECHOIC? |
Hypoechoic |
|
|
ON US, PLACENTA INFARCTS ARE UNABLE TO BE DISTINGUISHED FROM WHAT KIND OF HEMORRHAGE? |
Intraplacental hemorrhage |
|
|
OVER TIME, WHAT MAY OCCUR W/ PLACENTAL INFARCTS? |
Calcification |