![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
209 Cards in this Set
- Front
- Back
|
T/F: Primary shoulder OA is common |
False: it is much less common than OA of major joints in the lower limbs |
|
|
What movement is mostly affected by OA of the shoulder? |
External rotation (but all movements are affected) |
|
|
Name the common pathophysiological pathway of secondary OA of the shoulder |
Major tear of the rotator cuff tendon |
|
|
Confirmation of diagnosis of OA of the shoulder |
Plain radiographs of the shoulder showing loss of joint space and osteosclerosis |
|
|
Two typical management options of OA of the shoulder. When would each be performed? What's their impact on patient's function? |
Total shoulder replacement If there is reasonable bone stock and intact rotator cuff Better results Hemiarthroplasty If glenoid cavity or rotator cuff are deficient Reduces pain but ROM remains limited |
|
|
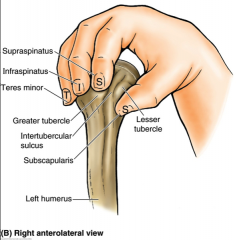
Where do rotator cuff attach? |
|
|
|
What is impingement syndrome? |
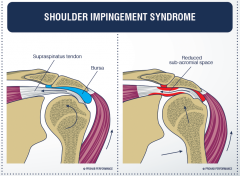
Compression of the rotator cuff tendon between the acromion of the scapula and the humerus. |
|
|
Typical presentation of impingement syndrome |
Pain on abduction of the shoulder from 45° to 120° |
|
|
Management of impingement syndrome (3) |
Natural resolution Steroid injection Surgical repair depending on underlying cause: Decompression of subacromial bursa or trimming of acromion by arthroscopy |
|
|
Demographics affected by frozen shoulder |
Middle age and elderly |
|
|
Pathogenesis of frozen shoulder (2 words) |
Capsular fibrosis |
|
|
Clinical presentation of frozen shoulder |
3 phases (6-12/12 each) 1) Pain and increasing stiffness 2) Stiff and less painful 3) Stiffness resolves |
|
|
X-ray findings in frozen shoulder |
None but seen on USS |
|
|
How is the diagnosis of frozen shoulder made? |
Clinically – Global loss of movements |
|
|
Which movement is most affected in frozen shoulder? |
External rotation (but all movements affected) (Like OA) |
|
|
Management of frozen shoulder (3) |
NSAIDs Physiotherapy Local steroid injection |
|
|
What does bilateral frozen shoulder suggest |
Diabetes (think of icecream eaters) |
|
|
23 year old presents with pain on abduction of the shoulder between 30 and 110° and reduced external rotation after a ski accident. Diagnosis? |
Rotator cuff tear (more likely than impingement due to the hx of trauma) |
|
|
One RF for frozen shoulder |
Diabetes |
|
|
Age group of OA, frozen shoulder and impingement syndrome |
OA – Elderly FS – Middle age and elderly IS – Middle age |
|
|
Direction of dislocation in Colles and Smith's fractures? |
There is no dislocation |
|
|
Direction of deviation and angulation in Colles and Smith's fractures |
Colles – Radial and dorsal displacement and angulation Smith – Volar displacement and volar angulation |
|
|
T/F: Both Smith and Colles fractures are extra-articular |
T |
|
|
Fixation of Colles' fracture |
Cast in palmar flexion and ulnar deviation with 3 point fixation |
|
|
What is Barton's fracture? |
Intra-articular fracture with radio-carpal dislocation |
|
|
Management of torus fractures? |
Innocuous ⟹ Splint |
|
|
T/F: Salter-Harris type 1 fracture are much more common in children |
T: Slipping occurs when growth plate has not fused |
|
|
Most likely direction of dislocation of the hip, shoulder, knee and elbow |
Shoulder – Anterior Elbow – Posterior Hip – Posterior Knee – Anterior Note that it is symmetrical since the anterior part of the lower limb is the posterior part of the upper limb |
|
|
Define the different classes of haemorrhagic shock |
Based on blood loss Type 1 < 0.75L (15%) Type 2 < 1.5L (30%) Type 3 < 2L (40%) Type 4 > 2L (40%) |
|
|
How do the following markers typically evolve with the severity of an haemorrhagic shock: HR BP Pulse pressure RR Urine output |
HR increases BP decreases PP decreases RR increases Urine output decreases |
|

|
Posterior elbow dislocation (see the olecranon) |
|
|
First line management of open fracture (if not actively bleeding) |
Sterile saline soaked dressing over it and photograph for medicolegal reasons |
|
|
Most common septic joint in children. What is the likely organism? What imaging would you use? Management? |
Septic hip Staph aureus USS US-guided aspiration and broad spectrum ABx |
|

|
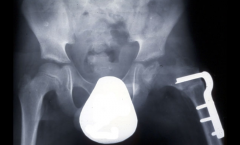
Developmental dysplasia of the hip |
|
|
Define Hilgenreiner's line |
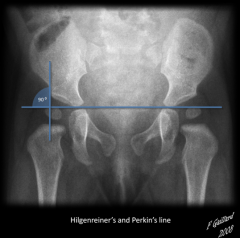
Line running between the inferior aspects of both triradiate cartilages of the acetabulums |
|
|
How is developmental dysplasia of the hip recognised on AP scan? |
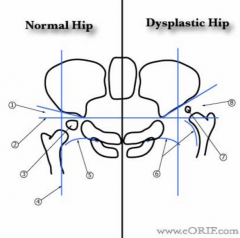
Small growth nucleus lies above the Hilgenreiner line |
|
|
What gender is most at risk of developmental dysplasia of the hip? |
Female because of more flexible ligaments |
|
|
4 RF for developmental dysplasia of the hip |
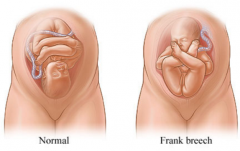
Breech Family history Oligohydraminos (not enough amniotic fluid) Female First born |
|
|
5 signs of developmental dysplasia of the hip |
Leg length discrepancy Reduced abduction and flexion Clunking Barlow (out – pushing on joined knees and adducting slightly to see if you can dislocate the hip) Ortalani (in – abduct the hip to tray and relocate the hip) |
|
|
Distinguish Barlow's sign and Ortalani's sign |

Both used to assess developmental dysplasia of the hip
|
|
|
What should be done if there is any suspicion of a developmental dysplasia of the hip |
Confirm with USS (if before 4/12 of age) or X-ray (if after 4/12) |
|
|
What is talipes equinovarus |

Scientific name for club foot |
|
|
Aetiology of club foot |
Idiopathic – The one requiring treatment Positional (due to position in uterus) – Can be passively brought back in place |
|
|
4 signs of club foot |
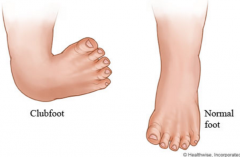
Cavus (midfoot) Adduction (forefoot relative to hindfoot) Varus (hindfoot) Equimus (like a horse, foot pointing down) |
|
|
Treatment of club foot |
Ponseti method Progressive alternation of reductions and casting for up to 8 weeks followed by tenotomy of Achilles tendon Passive repositioning If positional club foot |
|
|
Perthes disease – Avascular necrosis of femoral head |
|
|
What is Perthes disease? |
Emergency Idiopathic avascular necrosis of the femoral head |
|
|
Demographics at risk of Perthes disease |
Primary school girls |
|
|
Presentation of Perthes disease (3) |
Fatigue, pain (mostly knee), irritable hip with reduced ROM |
|
|
How does Perthes disease present on X-ray? |
Flattening of the femoral head |
|
|
Management of Perthes disease |
Rest Surveillance (X-ray) Surgery |
|
|
2yo non weight bearing on right leg, T°C = 38.8, WCC=17 and ESR=42. Diagnosis? |
Septic arthritis |
|
|
Diagnostic criteria for septic arthritis |
Kocher’s criteria Non-weight bearing T°C > 38.5 WCC>12 ESR>40 Points: 1 – 3% 2 – 40% 3 – 93% 4 – 99% |
|
|
Management of septic arthritis |
Emergency washout (within 6 hours) |
|
|
5 likely locations of primary tumour in bone mets |
Prostate Breast Kidney |
|
|
Investigation of choice for secondary bone tumours |
CT CAP |
|
|
Common site of the following tumours: – Osteosarcoma – Ewing's sarcoma |
Osteosarcoma – Metaphysis of long bones (mostly knee – 60%) Ewing's sarcoma – Metaphysis and diaphysis of long bones (femur, tibia, humerus) and flat bones (eg pelvis) |
|
|
Most common malignant tumour of bone |
Metastatic carcinoma |
|
|
Most common primary malignant tumour of bone |
Osteosarcoma |
|
|
Typical pt (epidemiology) with bone–forming tumour (osteoma, osteoid osteoma, osteosarcoma) |
Male teen/young adult |
|
|
Typical pt (epidemiology) with Ewing's sarcoma |
Male child/teen |
|
|
Symptoms of bone forming tumour |
Pain worse at night Swelling |
|
|
22 ♂ found with a mass on the superior aspect of the thigh that is hard and painful (wakes him during the night) and has been growing for the last year. Cytogenetic analysis of the tumour reveals mutation to RB1 and TP23. Diagnosis? |
Osteosarcoma |
|
|
22 ♂ found with a mass on the superior aspect of the thigh that is hard and painful (wakes him during the night) and has been growing for the last year. Histology reveals osteoblasts with pleomorphism, areas of haemorrhage and necrosis. Diagnosis? |
Osteosarcoma |
|
|
14 ♂ presents with swelling around his arm near the shoulder that has been progressively worse for the past 2 weeks. The area is also painful (particularly at night). WCC ➚ and ESR ➚. What is the differential and how will you establish a diagnosis? |
XR and thenBiopsy (to differentiate Ewing's sarcoma from osteomyelitis) |
|
|
14 ♂ presents with swelling around his arm near the shoulder that has been progressively worse for the past 2 weeks. The area is also painful (particularly at night). WCC ➚ and ESR ➚. Biopsy and cytogenetics reveals a 11–22 translocation. Diagnosis? |
Ewing's sarcoma |
|
|
True or false: Ewing's sarcoma are high grade tumour |
True (they are made of round cells) |
|

|
Osteosarcoma |
|

|
Osteosarcoma |
|
|
Ewing's sarcoma |
|

Which is what |

|
|
|
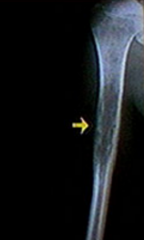
Three common features of Ewing's sarcoma on X-ray |
Permeation (76%) – Poorly defined "holes" within bone Laminated periosteal reaction (57%) – Onion skin Sclerosis (40%) |
|
|
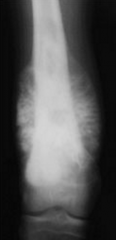
Three common features of osteosarcoma on X-ray |
Medullary and cortical destruction Permeation – Poorly defined "holes" within bone Aggressive periosteal reaction – Sunburst |
|
|
T/F: periosteal reaction (sunburst vs onion skin) enables distinction of Ewing's sarcoma from osteosarcoma |
True and False: both can present with both but Ewing's sarcoma most commonly present with onion skin while osteosarcoma most commonly present with sunburst |
|
|
Swelling in the knee that has been growing for years in a teenager with night pain. Likely diagnosis |
Osteosarcoma (60% occur in the knee) |
|
|
What imaging is used for staging of osteosarcoma |
Local staging by MRI (for skip lesions) prior to biopsy Distant staging with bone scan and chest CT |
|
|
Management of osteosarcoma |
Aggressive surgical resection (often with amputation) followed by chemotherapy |
|
|
Where do osteosarcoma metastasise (3)? |
Lungs Other bones Lymph nodes |
|
|
Management of Ewing's sarcoma |
Chemotherapy ± Surgery/Radiotherapy depending of the location and size of the tumour |
|
|
Which location of Ewing's sarcoma confer the worst prognosis? |
Pelvis |
|
|
Where do Ewing's sarcoma metastasise (2)? |
Lungs Other bones (Not lymph nodes, unlike Osteosarcoma) |
|

Name of the sign and disease where it occurs |
Codman's triangle Most commonly occur in osteosarcoma (but also in Ewing's sarcoma) |
|
Name of the sign and disease where it occurs |
Sunburst Most commonly occur in osteosarcoma (but also in Ewing's sarcoma) |
|

Name of the sign and disease where it occurs |
Onion skin Most commonly occur in Ewing's sarcoma (but also in osteosarcoma) |
|

|
Dupuytren's contracture |
|
|
Pathogenesis of Dupuytren's contracture |
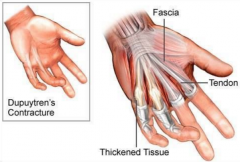
Contraction of palmar fascia so that fingers (mostly little and ring fingers) cannot contract |
|
|
What joints are affected by Dupuytren's contracture |
MCP and sometimes PIP/DIP |
|
|
Management of Dupuytren's contracture |
Surgery (fasciotomy) if MCP contracture > 30° or PIP/DIP contracture > 10° If caught too late, amputation of the fingers (that are on the way) can be considered |
|
|
Demographic affected by Dupuytren's contracture |
Males > 65 |
|
|
Ottawa rules for foot x-ray |
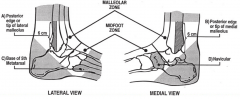
Pain in the midfoot zone and any one of the following A) Bone tenderness over base of 5th metatarsal B) Bone tenderness over navicular C) Inability to bear weight both immediately and in the emergency department for four steps |
|
|
Ottawa rules for ankle x-ray |
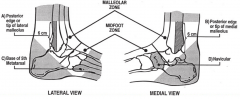
Pain in the malleolar zone and any one of the following A) Bone tenderness along the distal 6 cm of the posterior edge of the tibia or tip of the medial malleolus B) Bone tenderness along the distal 6 cm of the posterior edge of the fibula or tip of the lateral malleolus C) Inability to bear weight both immediately and in the emergency department for four steps |
|
|
Ottawa rules for knee x-ray |
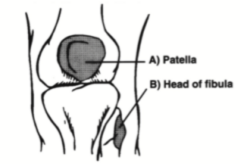
Knee injury and any of the following A) > 55 B) Tenderness in patella only C) Tenderness at head of fibula D) Inability to flex at 90° E) Inability to bear weight both immediately and in the emergency department for four steps |
|
|
Patient presents with back pain. O/E there is saddle anaesthesia. Name one possible diagnosis, one other sign and two elements of immediate management. |
Cauda equina syndrome Reduced anal tone on PR Urgent MRI and steroids |
|
|
Where can you test dermatomes of L4, L5 and S1 |
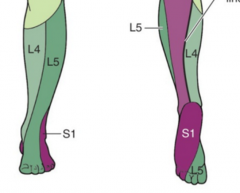
L4 – Medial malleolus L5 – 1st dorsal webspace on foot S1 – Outside little toe/plantar side |
|
|
Patient with back pain and saddle anaesthesia is found to have lost sensation over the lateral aspect of his lower leg and over big toe but intact sensation over medial malleolus. Where is the lesion if this is cause by disc prolapse? |
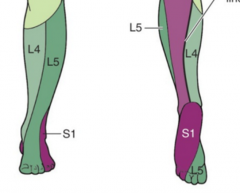
L4/5 prolapse impairing L5 but preserving L4 nerve roots. |
|
|
Where can you test the peripheral dermatomes of the radial, median and ulnar nerves? |
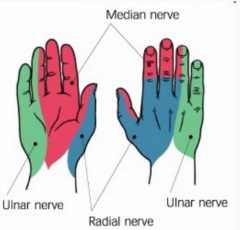
Radial – 1st webspace (dorsal) Median – Index (palmar) Ulnar – Little (palmar) |
|
|
T/F – Posterior interosseous nerve only carries sensory information |
False: it only carries motor information |
|
|
What structure is at risk when there is humeral fracture |
Radial nerve |
|
|
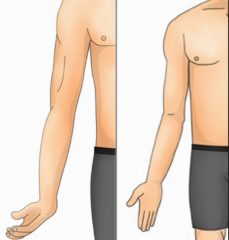
Name and describe two tests that can be used to diagnose carpal tunnel syndrome. |
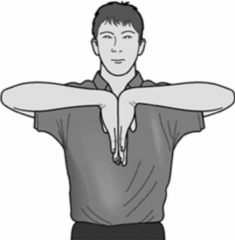
Phalen's test (displayed) Hold in position for 1min Positive if symptoms of CTS are exaggerated/elicited Tinel's test Tapping over the carpal tunnel causes paraesthaesia |
|
|
How can carpal tunnel syndrome be confirmed if in doubtM? |
Nerve conduction study |
|
|
10 causes of carpal tunnel syndrome |
ICRAMPS (Cx2, Ax2, Mx3, Sx2) Idiopathic |
|
|
Dermatome and myotome of median nerve |
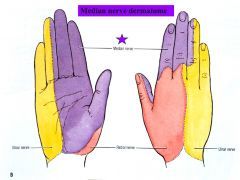
1/2 LOAF Lumbricals 1 and 2 Opponens pollicis Abductor pollicis brevis Flexor pollicis brevis |
|
|
Boundaries of the carpal tunnel |
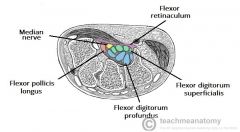
Floor – Carpus (scaphoid, trapezium, pisiform, hook hamate) Roof – Flexor retinaculum |
|
|
Content of the carpal tunnel |
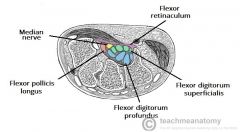
Median nerve Flexor digitorum superficialis Flexor digitorum profundus Flexor pollicis longus |
|
|
Management of carpal tunnel syndrome |
From first line to third line 1) Night splint 2) Steroid injection 3) Orthopaedic referral for division of flexor retinaculum |
|
|
Name the rotator cuff muscles, their peripheral innervation and nerve root(s) |
Supraspinatus and Infraspinatus Suprascapular nerve – C5,6 Subscapularis Subscapular nerve – C5,6 Teres minor Axillary nerve – C5,6 |
|
|
Pattern recognition Structures at risk if you fall from height (2) |
Calcaneus Thoracic vertebrae |
|
|
Pattern recognition Structures at risk in dashboard injury (3) |
Posterior hip dislocation Posterior cruciate ligaments Patellar fracture |
|
|
Pattern recognition Structure at risk in motorbike accident |
Brachial plexus (upper trunk) |
|
|
Signs of injury to the upper trunk of the brachial plexus |
Erb's palsy |
|
|
What fraction of hip replacement are functioning at 10 years? 20years? |
90% at 10 years 80% at 20 years |
|
|
Compare complications of hip and knee replacements (4) |
Hip Dislocation Leg length discrepancy Infection Aseptic loosening Knee No dislocation No leg length discrepancy Infection Aseptic loosening |
|
|
What is aseptic loosening |
Failure of the bond between an implant and bone in the absence of infection. |
|
|
What does the ACL and PCL connect and what movements do they restrain? |
ACL Medial tibia to lateral femur Prevents anterior translocation of tibia on femur PCL Lateral tibia to medial femur Prevents posterior translocation of tibia on femur |
|
|
T/F: ACL prevents posterior translocation of femur on tibia |
True: this is equivalent to anterior translocation of tibia on femur |
|
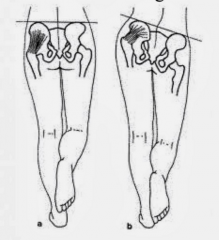
Name that sign. Why and when does it occur? Which side is affected? |
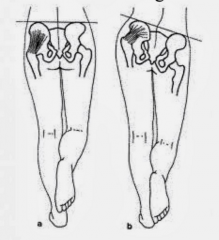
Trendelenburg's sign Left leg is affected Caused by weak left abductors that normally keeps the hip straight. |
|
|
Which muscles enable normal abduction of the hip when walking? What is their innervation |
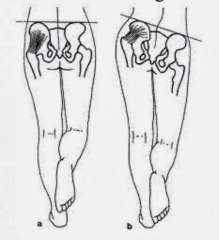
Glutenus medius and minimus – Superior gluteal nerve (lesion to this nerve causes positive Trendelenburg's sign) |
|
|
What structures can be damaged when there is volar cut to the wrist (9) |
Flexor tendons Flexor digitorum superficialis Flexor digitorum profundus Flexor carpi ulnaris Flexor carpi radialis Flexor pollicis longus Palmaris longus tendon (not always present) NV Ulnar nerve Median nerve Ulnar artery (Radial artery runs deeper and more laterally) |
|
|
Outline the motor, sensory, and autonomic symptoms of cauda equina syndrome |
Motor Flaccid leg weakness and decreased anal sphincter tone on PR Reflexes Absent in the leg Sensory Loss in root distribution and low back pain Autonomic Constipation, urinary retention, impotence (think PNS symptoms) |
|
|
Most common aetiology of cauda equina |
Herniated disc |
|
|
Does cauda equina syndrome cause SNS lesion or PNS lesion symptoms? Why? |
PNS lesion symptoms: constipation, urinary retention, impotence Because the PNS nerves to the abdominal viscera emerge from S2–S4 which are part of the cauda equina whereas the most caudal SNS nerves emerge from L2 which is just at the upper limit of the cauda equina so unless the lesion is at the top of the cauda equina (very unlikely), no SNS nerve will be damaged while all PNS nerves may be affected. Remember also that the most likely cause for cauda equina syndrome is massive disc herniation and that the most likely discs to herniate are L4–L5 and L5–S1, both of which would affect all PNS. |
|
|
What element of history (2) and examination (3) would suggest cauda equina in a patient with back pain? |
Hx Saddle anaesthesia Sphincter dysfunction (urinary of faecal incontinence) Examination Severe or progressive lower limb neurological deficit Unexpected laxity of the anal sphincter Perianal/Perineal sensory loss |
|
|
Where does the cauda equina begin? |
L1/L2 |
|
|
Besides disc herniation, name 3 other causes of cauda equina syndrome |
Spinal stenosis Infection/Inflammation within spinal canal Tumour Spinal injury |
|
|
Significance of bilateral signs in cauda equina syndrome |
Central disc prolapse |
|
|
Management of cauda equina syndrome |
Emergency MRI to confirm diagnosis Urgent (asap) surgical decompression by removing the disc |
|
|
Patient presents with a finger that appears perfectly normal. However, when flexing it, a click is heard and the finger is stuck in its flexed position. Name of the condition, pathogenesis, management. |
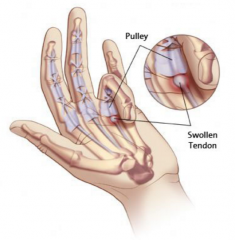
Name Trigger finger Pathogenesis Thickening of the flexor tendon so that tendon does not move freely in and out of the tunnel from palm to finger. Management Steroid injection Surgical opening of the mouth of the tendon tunnel |
|
|
3 RF for trigger finger |
Repeated trauma to palm RA DM |
|
|
T/F: the triggered finger can be brought back to its position by the other hand |
Trye |
|
|
Most common fingers to present with trigger finger (2) |
Ring and middle |
|
|
What triggers the development of frozen shoulder? |
Strenuous use of the shoulder (eg painting a ceiling) or injury to shoulder |
|
|
Pattern recognition 50 year old lady cannot move her shoulder following two days painting the ceiling |
Frozen shoulder |
|
|
Pattern recognition Pain occurring in a limited arc of abduction of the shoulder without history of trauma (60–120°—painful arc syndrome) |
Impingement syndrome |
|
|
What causes impingement syndrome? |
A) Inflammation of the subacromial bursa which often occurs after exercise in middle age individuals. B) Beaking of the underside of the acromion due to aging. |
|
|
What makes the repair of rotator cuff injury difficult? |
They have poor blood supply so healing is often compromised |
|
|
Pattern recognition Trauma with painful arc |
Rotator cuff tear |
|
|
Pattern recognition Diabetic middle age with hx of shoulder pain that is now stiff but no more painful |
Frozen shoulder |
|
|
What rotator cuff problem may occur following shoulder dislocation? |
Rotator cuff tear |
|
|
Investigation in rotator cuff tear |
X-ray to rule out fractures Then MRI or USS to delineate the tendons of the rotator cuff |
|
|
Management of rotator cuff tear |
Refer for orthopaedic surgery (open or arthroscopic) |
|
|
How is developmental dysplasia of the hip corrected if caught early? if left to later in life? |
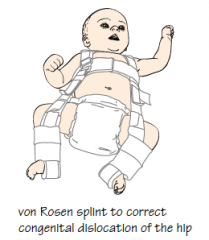
Early Splints that hold the hip in abduction and internal rotation so that the femoral head grows within the acetabulum Late Surgical repair |
|
|
In practice, how is developmental dysplasia of the hip diagnosed? |
A) High risk babies (breech or family history) ⟹ Screening with USS in the first 2/12 of life B) Part of the clinical screening of newborn C) Undetected, presents with limp or frequent falls |
|
|
Most common complication of Perthes disease |
Early arthritis |
|
|
Pattern recognition 14yo boy obese with pain at rest in the knee and a limp. What should you exclude? |
Slipped upper femoral epiphysis (SUFE) |
|
|
Pattern recognition 14yo boy tall and slim with pain at rest in the knee and a limp. What should you exclude? |
Slipped upper femoral epiphysis (SUFE) |
|
|
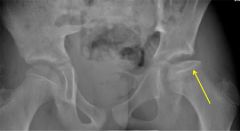
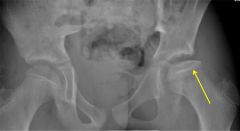
What is slipped upper femoral epiphysis (SUFE)? |
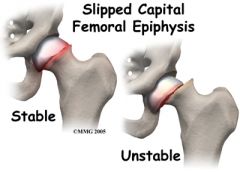
Femoral epiphysis slips with respect to the femur usually in a postero-inferior direction |
|
|
What movements are impaired in slipped upper femoral epiphysis? |
Most hip movements, particularly abduction and internal rotation |
|
|
How may the leg appear in a patient with slipped upper femoral epiphysis (2)? |
Shortened and externally rotated |
|
|
What demographics is mostly affected by SUFE? |
Teenage boys (10-15) |
|
|
Management of slipped upper femoral epiphysis |
1) Confirm with X-ray 2) Surgical pinning or reconstructive surgery 3) Monitor other hip |
|
|
3 complications of slipped upper femoral epiphysis |
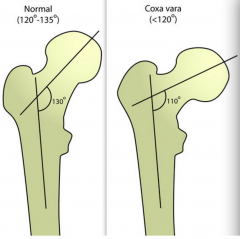
Avascular necrosis Coxa vara Early osteoarthritis |
|

|
Slipped upper femoral epiphysis on the left |
|
|
T/F: Bilateral SUFE is common |
True (20%) |
|

|
Syndactyly |
|
|
Management of syndactyly |
Separation and skin grafting at 4y (only for cosmetic reasons) |
|

|
Cerebral palsy |
|
|
Define cerebral palsy |
Injury of any sort (mechanical, hypoxic...) to immature brain (< 2y) resulting in upper motor neurone disease |
|
|
How does cerebral palsy present (evolution) |
1°) Floppy 2°) Slow development 3°) Spasticity of variable parts of the body |
|
|
T/F: Intelligence is often affected in children with cerebral palsy |
False: in many cases it is intact but motor retardation acts as a false positive |
|
|
T/F: Cerebral palsy is a progressive disease |
False: although its manifestations may change with development of the child |
|
|
What is spasticity? |
Increased tone that is velocity-dependent |
|
|
Besides spasticity, what other 3 motor abnormality can be present in cerebral palsy? |
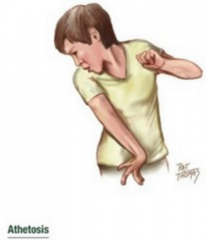
Athetosis Ataxia Rigidity |
|
|
Management of cerebral palsy at the spastic stage (2) |
Stretching Botulinum toxin Most importantly: try to enable the child to get as much out of life as possible |
|
|
Two long term complications of cerebral palsy and their management |
Muscle shortening ⟹ Serial casting, botulinum toxin, muscle lengthening surgery Secondary bone changes ⟹ Osteotomy |
|
|
|
|
|
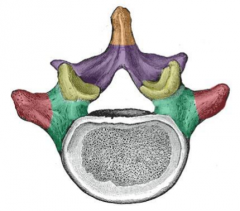
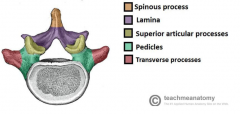
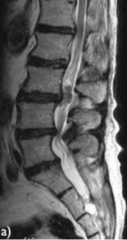
Outline the structure of vertebral discs. What prolapses in prolapse disc? |
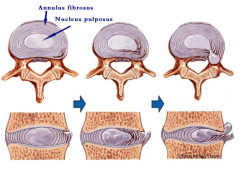
Nucleus pulposus prolapses through a rupture in the annulus |
|
|
3 outcomes of disc herniation |
Compression of a nerve root Compression of the spinal cord Compression of the cauda equina |
|
|
How does compression of the nerve root present? |
Radiculopathy – Shooting pain, numbness and weakness in the distribution of the affected nerve |
|
|
What is sciatica? |
Radiculopathy (due to compression of a nerve root) in the root supplying the sciatic nerve (L4-S3) |
|
|
Describe the sensory, motor and reflex affected by compression of L4, L5 and S1. |
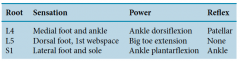
|
|

|
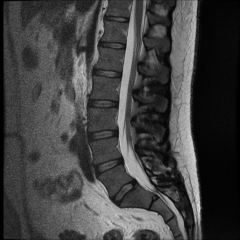
Normal spine |
|

|
Normal spine |
|

|
Herniated disc |
|
|
Herniated disc |
|
|
Normal spine |
|
|
Management of herniated disc |
Analgesia Investigate for cauda equina syndrome (confirm with MRI if needed) |
|
|
75 year old man with leg pain that are worse on walking and standing and relieved by lying flat. Two differentials and how you will distinguish them |
Claudication (abnormal vascular exam) Spinal stenosis (normal vascular exam) |
|
|
What causes spinal stenosis? |

Combination of disc herniation and arthritis of the facet joints at the back of the spine |
|
|
Pattern recognition Leg pain when walking but better when walking in a supermarket |
Spinal stenosis (leaning on the trolley helps opening the spinal canal) |
|
|
Treatment of spinal stenosis (2) |
Epidural steroid injection or Surgical decompression by laminectomy (removing back of one or more vertebrae) |
|
|
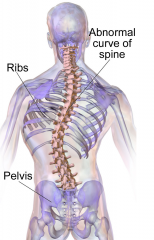
Scoliosis |
|
|
Significance of scoliosis that disappears on bending forward |
Postural scoliosis: no clinical significance |
|
|
3 clinical signs of scoliosis |
Spinal curvature Difference in shoulder height Difference in space between trunk and upper limbs |
|
|
Scoliosis with night pain. What should you do? |
Suspect cancer ⟹ Refer urgently to orthopaedics |
|
|
3 RF for scoliosis |
Adolescent of tall parents who are growing fast |
|
|
Management of idiopathic scoliosis |
Depends on individual. Rule of thumb – Cobb angle < 25° – Observe 25°-40° – Brace > 40° – Consider surgery |
|
|
T/F : Scoliosis is curvature of the spine in the coronal plane |
False, curvature occurs in all 3 planes: rotation (axial), lateral bending (coronal) and lordosis (sagittal) |
|
|
Most common deformity observed in scoliosis |
Right thoracic curve |
|
|
Why is it difficult to assess scoliosis in patients? What can be done about it? |

It tend to be compensated for thoracic bend by bending the lumbar spine.
|
|

|
Bunion |
|
|
What is hallux valgus? |
Scientific term for bunion which also explains the pathogenesis: distal part of big toe bends laterally |
|
|
Pathogenesis of bunion |

Lateral bending of big toe leaving a prominent head of the metatarsal bone which forms a bursaover it while the skin becomes inflamed |
|
|
Management of bunion |
Conservative – Adapted shoewear Surgery – Osteotomy through the metatarsal and removal of the bursa |
|
|
RF for bunion |
Women wearing narrow shoes |
|

|
Claw toes |
|
|
What are claw toes |

|
|
|
What causes claw toes? |

Inflammatory joint disease (eg RA) causing dorsal dislocation of the metatarso-phalangeal (MTP) joint and flexion of the PIP and DIP joints |
|
|
How do patients with claw toes present? Name the main symptom |

Metatarsalgia Metatarsal heads become very painful to walk on ("It feels like walking bare foot on pebbles (cailloux)") |
|
|
Management of claw toes |
Surgery to straighten the toe and bring a thick pad of tissue over the metatarsal heads + Padded shoes |
|
|
3 deformities present in claw toes |

Extension of MTP Flexion of DIP and PIP |
|
|
Beside claw toes, name 4 causes of metatarsalgia |
Synovitis Stress fracture Sesamoid fracture Injury |
|
|
Define flat feet and describe a test to confirm it |
Complete failure of the foot to form an arch Windlass test (picture) – Dorsiflex the toes (or ask patient to stand on toes). Positive if still no arch. |
|
|
Name and describe one congenital cause of flat feet |
Tarsal coalition Abnormal connections betweenbones of the foot resulting in rigid foot deformity: |
|
|
Two most common forms of tarsal coalition and their presentation on radiographs |
Calcaneonavicular coalition (40%) – Ant-eater Talocalcaneal coalition (50%) – C-sign |
|

|
C sign – Bony connection between talus and calcaneum in tarsal coalition |
|

|
Ant-eater sign – Bony connection between navicular and calcaneum in tarsal coalition |
|
|
T/F – Congenital tarsal coalition present in young children |
False – During early childhood, cartilage is flexible and coalition is therefore silent. CTC thus mostly presents in 20s. |
|
|
Investigation of congenital tarsal coalition |
X-rays showing C-sign (Talocalcaneal coalition) or ant-eater sign (Calcaneonavicular coalition) |
|
|
Management of tarsal coalition |
Rest in a cast for 6 weeks to resolve ankle pain If it fails, surgical resection of coalition |