![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
223 Cards in this Set
- Front
- Back
|
Rule for automatic acceptance in major trauma centre in poly trauma? |
A, B or C A) Haemodynamic instability B) Visceral laceration ⊙ fractured (long bone/pelvis/spine) C) Significant injury ⊙ Injury requiring specialty care at major trauma centre |
|
|
Rule for automatic acceptance in major trauma centre in neuro trauma? |
A or B A) Penetrating head injury B) Head injury with CT changes |
|
|
Rule for automatic acceptance in major trauma centre in spine trauma? |
A) Unstable spinal injury (any level) B) Spinal injury with neurology C) Open spin fracture |
|
|
Rule for automatic acceptance in major trauma centre in thoracic trauma? |
A) Penetrating chest injury B) Flail chest in ≥3 segments C) Rupture bronchus or diaphragm D) Blood loss of >0.5L immediately following insertion of chest drain or 0.25L/hour for ≥3h D) Suspected aortic transection E) Cardiac tamponade |
|
|
Rule for automatic acceptance in major trauma centre in pelvis trauma? |
Haemodynamic instability Pelvic or acetabular fracture requiring surgery |
|
|
Rule for automatic acceptance in major trauma centre in extremities trauma? |
De-vascularised limb Open fracture of lower limb or (upper limb ⊙ requiring debridement/soft tissue cover) |
|
|
Rule for automatic acceptance in major trauma centre in burns? |
Multiple injuries ⊙ burn injury |
|
|
How is the Major Trauma Centre contacted? |
Call 2222 and state "Adult trauma call to JR ED Resus" |
|
|
To whom is the call transferred when 2222 is called with "Adult trauma call to JR ED Resus" is activated and what is her/their role? |
Crash bleep of... Trauma FY2 (Scribe) Trauma registrar (Primary survey) ICU registrar (Airway) General surgeon registrar Surgery SHO ED senior (Trauma Team Leader) |
|
|
True or false: imaging can hopefully be acquired and analysed faster in a case of a trauma call because the radiographer and radiologist are also paged following 2222 call |
True |
|
|
Which number should be called to activate Major Haemorrhage Pack? |
4444 |
|
|
Patient is actively bleeding large amounts. What should you do? |
1) Administer tranexamic acid (TXA) - 1g bolus followed by 1g infusion 2) Call switchboard on 4444 3) Request MHP Pack 1 4) Take blood and send to lab while waiting: X-match, FBC, PT, aPTT, Fibrinogen, U&E, Ca (2 purple, 1 blue, 1 green) 5) Give MHP Pack 1 6) Reassess |
|
|
What does the Major Haemorrhage Protocol Pack 1 contain? |
6 units of RBC 4 units of FFP Emergency O blood if required |
|
|
What is the deadly triad of a patient who is bleeding? |
Hypothermia Acidosis Coagulopathy |
|
|
Why is it important to minimise movements in major trauma? |
Avoid dislodging a clot which would cause haemorrhage |
|
|
Patient with major trauma has been stabilised with ABC. What is the next step in investigation? |
CT Trauma scan (head/neck/thorax/abdo/pelvis with contrast) |
|
|
Patient has sustained trauma and has reduced consciousness level (GCS = 7). What do you do regarding airways? |
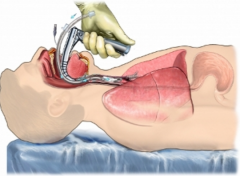
Endotracheal intubation since airway reflexes have been lost |
|
|
AVPU and GCS threshold for endotracheal intubtaion |
AVPU ≤ P |
|
|
What is triple immobilisation in trauma? |

Cervical collar Blocks placed on both side of the head Tape across the forehead and chin |
|
|
Name 6 chest emergency that may cause death due to impaired breathing |
Airway obstruction (transection of bronchus) Tension pneumothorax Open pneumothorax Massive haemothorax Flail chest Cardiac tamponade |
|
|
Management of open pneumothorax |
Close wound and chest drain If not available: place a bandage and attach it at three corners creating a one-way valve allowing air to escape during expiration. |
|
|
Diagnosis of cardiac tamponade |
USS |
|
|
What defines severe traumatic brain injury and moderate TBI? |
Severe TBI: GCS ≤ 8 Moderate TBI: 9 ≤ GCS ≤ 12 |
|
|
Define cerebral perfusion pressure |
Mean arterial pressure - ICP |
|
|
Patient has a GCS of 7. You achieve endotracheal intubation and start ventilation. But the patient keeps deteriorating. What do you do? |
Mannitol + Hyperventilation |
|
|
What clinical sign may suggest coning? |
Cushing's triad Bradycardia Hypertension Irregular breathing |
|
|
Describe the Glasgow Coma Scale |

|
|
|
True or false: trauma is a disease |
True since a disease is a particular abnormal condition, adisorder of a structure or function, that affects part orall of an organism. |
|

|
|
|
|
Define fracture |
Break or discontinuity in the cortex of a bone |
|
|
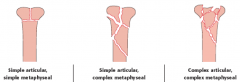
Outline the 5 step description of fractures |
1) Bone 2) Part of the bone 3) Type of fracture a. Simple (spiral, oblique transverse) b. Wedge c. Complex d. Intraarticular 4) Deformity a. Translation b. Angulation c. Rotation d. Shortening 5) Soft tissues and joints: a. Open/Closed b. Joint (dislocated, subluxated) c. Neurovascular status |
|
|
3 types of extra-articular fractures |

|
|
|
3 types of partially articular fractures |

|
|
|
3 types of articular fractures |
|
|
|
For extra-articular fractures, name: 3 simple 3 wedge 3 complex fractures |

|
|
|
5 broad approaches of fracture management |
1) Non-surgical external immobilisation (eg POP) 2) Surgical external fixation (eg frames) 3) Internal fixation: extramedullary (eg plate) 4) Internal fixation: intramedullary (eg nail) 5) Replacement |
|
|
3 ✔ and 3 ✘ of external immobilisation of fractures |
✔ Cheap ✔ Quick ✔ No surgery ✘ Muscle disuse ✘ Joint stiffness ✘ Inability to weight bear |
|
|
3 ✔ and 3 ✘ of surgical external fixation of fractures |
✔ Reduced surgery ✔ Reduced soft tissue damage ✔ Increased rigidity ✘ Pin site infection ✘ Cosmetics ✘ Unable to weight bear ✘ Uncomfortable ✘ Long healing |
|
|
4 main ✔︎ and 1 major ✘ of surgical approaches (internal fixation) of fractures |
✔ Improved control and stability ✔ Improved restoration of anatomy ✔ Earlier return of function ✔ Cosmetics ✘ Infection |
|
|
What is a patient with patent foramen ovale at risk of in fractures? |
Fat emboli leading to strokes (embolus forms in the veins and bypasses the pulmonary circulation to go to systemic circulation) |
|
|
Name 4 goals of fracture reduction from most to least urgent |
1) Reduce pain 2) Avoid neurovascular compromise and prevent further fat emboli 3) Restore function 4) Cosmetic |
|
|
4 steps in fracture reduction |
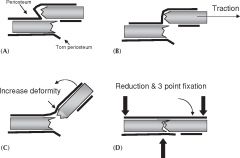
1) Exaggerate the deformity 2) Reverse mechanism of injury 3) Reduce 4) Three-point fixation (2 on the side distal to injury) |
|
|
Why is fracture of the pelvis particularly worrying? |
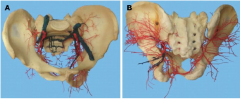
Because up to 2L of blood can be lost. If the blood is lost from a vein, then a clot should form. But, if the pelvis opens at the pubic symphysis ⟹ Pelvic volume increases ⟹ Pelvic pressure decreases ⟹ Clotting decreases ⟹ First thing to do is to close it asap to guarantee clotting If the blood is lost from an artery (or too big a vein), then clots don't form. |
|
|
Define open fracture |
A break in the skin and underlying soft tissueleading directly into or communicating with thefracture and its hematoma |
|
|
What is the Gustillo and Anderson classification useful for? |
Prognosis of open fracture (Level I is best, IIIC is worst) |
|
|
T/F: Inside-out open fractures are usually of better prognosis that outside-in |
True |
|
|
What is the periosteum? |
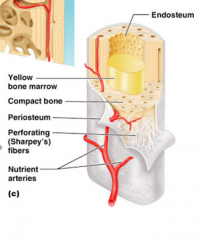
Dense layer of vascular connective tissue enveloping the bones except at the surfaces of the joints |
|
|
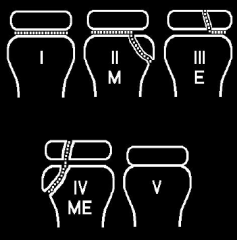
Outline (roughly) the pathological features of the Gustillo and Anderson classification of open fracture |
I – Inside-out injury II – Outside-in IIIa – II with extensive soft tissue laceration IIIb – IIIa with periosteal stripping and bone exposure |
|
|
8 steps of open fracture management |
1. Stop bleeding 2. Neurovascular assessment 3. Debride 5. Antibiotics 6. Tetanus assessment and active + passive immunisation if non-immunised 7. Take a picture 8. Splint |
|
|
Define compartment syndrome |
Raised pressure within a closedosteofascial compartmentresulting in tissue ischaemia andnecrosis |
|
|
Pathogenesis of compartment syndrome |
Compartment pressure ➚ ⟹ Capillary blood flow ➘ ⟹ Oedema ⟹ Pressure ➚ even more ⟹ Venous flow and lymphatic drainage ➘ ⟹ Pressure ➚ even more ⟹ Arteriolar blood flow ➘ ⟹ Ischaemia and necrosis |
|
|
Clinical criteria for the diagnosis of compartment syndrome |
Compartment pressure between 30 and 45mmHg (upper limit set because higher pressure suggests the probe is misplaced) |Compartment pressure - DBP| < 30mmHg |
|
|
How often should the compartment pressure be assessed in compartment syndrome? |
Every 30min |
|
|
Treatment of compartment syndrome |

Fasciotomy |
|
|
Early management of compartment syndrome while waiting for fasciotomy? |
1) Elevate leg above the heart 2) Analgesia 3) Review compartment pressure in 30min 4) Ice 5) Anti-inflammatory 6) Give a lot of O2 to avoid acidosis 7) Monitor the required morphine as increasing PRN is a sign of compartment syndrome |
|
|
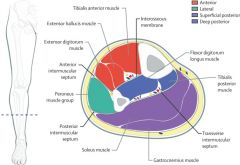
Outline the compartments of the lower leg and their content |
|
|
|
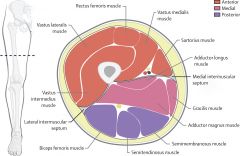
Outline the compartments of the thigh and their content |
|
|
|
When should dislocated joint be reduced? |
ASAP |
|
|
In which direction do hip mostly dislocate? How about shoulder? |
Hip – Posteriorly (90%) Shoulder – Anteriorly (90%) |
|
|
4 features of dislocated hip on XR |

Femoral head lateral and superior to acetabulum # posterior rim of acetabulum Femur in internal rotation and adduction Femoral head appear smaller due to magnification (AP scan) |
|
|
One common NV complication of hip dislocation and its clinical manifestation. Ho common is it? |
Sciatic nerve injury (10% of dislocations) Sensation – Foot, lower leg (apart from medial side) Muscles – Flexion of the knee, foot inversion and plantar flexion |
|

|
Knee dislocation |
|
|
What ligament(s) must be damaged to cause knee dislocation? |
Typically all four: ACL, PCL, MCL, LCL |
|
|
What NV structures are at risk of damage in knee dislocation (2)? For nervous structure, outline the clinical features. |
Popliteal artery – 10% (40% in anterior/posterior dislocations) Common peroneal nerve – 25% Foot drop Sensory loss in dorsum of foot |
|
|
T/F: knee dislocation can occur with low energy ligament if there is an axial component |
False: it mostly occurs in high-energy impact and occurs in low energy impact if there is rotational component |
|

|
Patella dislocation |
|
|
Which gender and which morphologies are most at risk of patella dislocation? |
Tall females |
|
|
Most likely direction of dislocation of patella |
Laterally |
|
|
How are patellar dislocations reduced? |
Hyperextension of the knee and medialward pressure on patella |
|
|
Indication for surgery in patellar dislocations |
If it occurs with very minor (eg walking) indicating a structural defect |
|
|
What forced movement causes anterior shoulder dislocation? |
Abduction + External rotation |
|
|
Patient complains of pain in the shoulder after seizure. Likely diagnosis |
Posterior shoulder dislocation |
|
|
Patient complains of pain in the shoulder after playing rugby. Likely diagnosis |
Anterior shoulder dislocation (abduction + external rotation) |
|
|
Patient complains of pain in the shoulder after FOOSH. Likely diagnosis |
Anterior shoulder dislocation (abduction + external rotation) |
|
|
Patient complains of pain in the shoulder after electric shock. Likely diagnosis |
Posterior shoulder dislocation |
|
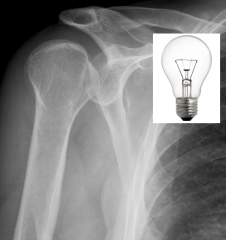
Patient complains of pain in the shoulder. XR reveals light bulb appearance. Likely diagnosis |
Posterior shoulder dislocation |
|
|
Why do electric shock and seizures cause posterior shoulder dislocation rather than the more common anterior shoulder dislocation? |
Because they cause powerful pectoral muscles to contract, causing internal rotation of shoulder which puts it in a position to dislocate posteriorly. |
|

|
Posterior shoulder dislocation (light bulb appearance) |
|

|
Anterior shoulder dislocation |
|
|
Common NV complication of anterior shoulder dislocation and its manifestations |
Axillary nerve damage Motor – Difficulty abducting shoulder after 15° Sensation – Loss in regimental badge area |
|
|
What two muscles are responsible for abduction of the shoulder? |

Supraspinatus – 0-15° Deltoid – 15-90° |
|
|
Name 4 complications of shoulder dislocation. For each, state the condition in which they occur. |

Bankart lesion Injury of anterior (inferior) glenoid labrum Condition: anterior shoulder dislocation Depression in the cortex of the posterolateral head of the humerus Condition: anterior shoulder dislocation Greater tuberosity fracture Axillary nerve damage |
|
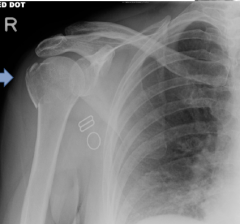
What complication of shoulder dislocation is demonstrated? |
Fracture of greater tuberosity |
|
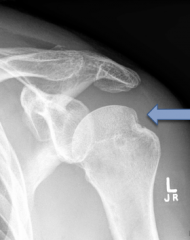
What complication of shoulder dislocation is demonstrated? |
Hill-Sachs lesion |
|

What complication of shoulder dislocation is demonstrated? |
Bony Bankart (look at the small fragment at the inferior aspect of the glenoid) |
|
|
Name and describe two techniques for shoulder reduction |
Modified Milch technique 1. Analgesia: entonox (50% NO, 50% O2) ± lidocaine injection 2. Patient supine, surgeon stands on side of affected arm and apply traction gently until patient "gives". 3. Abduct and externally rotate arm into overhead position Pull on arm hanging from chair (picture) |
|
|
|
|
|
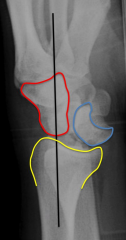
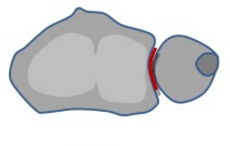
What is a perilunate dislocation? What articulation is affected? |
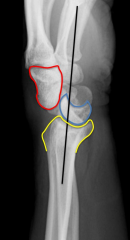
Capitate dislocated wrt lunate but lunate-radius articulation is intact. Red: Capitate Blue: Lunate Yellow: Radius |
|
|
What is a lunate dislocation? What articulation is affected? |
Lunate dislocated with respect to both the capitate and the radius Blue: Lunate Yellow: Radius |
|
|
What condition often co-occurs with perilunate dislocation? |
Trans-scaphoid fracture (60%) |
|
|
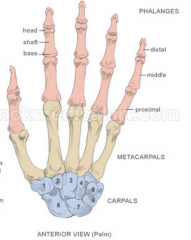
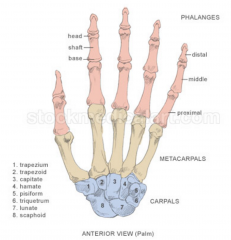
How can the alignment of carpals be assessed in XR? |
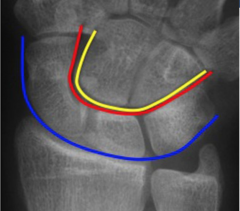
Gilula's lines Blue – Proximal edge of scaphoid, lunate, triquetrum
Red – Distal edge of scaphoid, lunate, triquetrum Yellow – Proximal edge of capitate and hamate Gilula's lines must be smooth, otherwise, there is likely injury |
|
|
Which of lunate and perilunate dislocations are most common? |
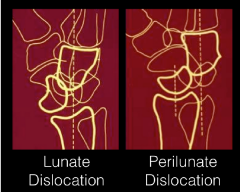
Perilunate |
|
|
What aspirates can you aspirate in the elbow (3) and in the knee (4) |
Elbow and knee Blood Pus Fat Knee Turbid fluid (crystals) |
|
|
Knee aspiration landmarks |

Lateral or medial to patella |
|
|
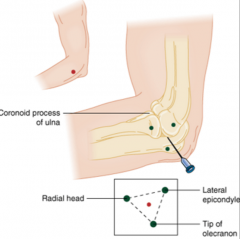
Elbow aspiration landmarks |
|
|
|
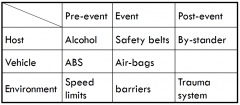
What is Haddon's matrix for road traffic collision prevention? |
|
|
|
4E of prevention synthesis |
Education (teach not to do) Enforcement (makes it illegal) Engineering (makes it impossible) Economics (discourage) |
|
|
4 types of non-accidental injury |
Neglect Physical Sexual Emotional |
|
|
T/F: non-accidental injury is the commonest cause of injury in < 4y |
T |
|
|
T/F: the commonest cause of broken femur in a 9m old child is fall |
False: it's non-accidental injury |
|
|
Commonest cause of fractures in < 1y |
Non-accidental injury |
|
|
For each of the following level of investigation, name a feature consistent with non-accidental injury: History General exam Exam of the injury |
Hx – Inconsistent Exam – Multiple bruises/injuries of differing ages Exam of injury – Long bone #, corner # (=bucket handle #) |
|
|
Management of non-accidental injury (5) |
1) Tell senior and safeguarding lead 2) Check child protection register 4) Paediatric review 5) Skeletal survey |
|
|
What is IMPS |
Injury minimisation programme for schools A program in which pupils at school are taught to do CPR, rescue breaths and use defibrillators |
|
|
T/F: as part of the IMPS, pupils are taught to do CPR, rescue breaths and use defibrillators |
True |
|
|
What is PTC |
Primary Trauma Care A foundation that provides training for trauma care in resource-poor environments |
|
|
Define inclination of the hip. What's its normal value? |
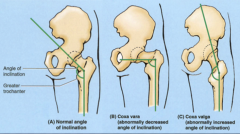
Normal: 130±7° |
|
|
Define anteversion of the hip. What's its normal value? |
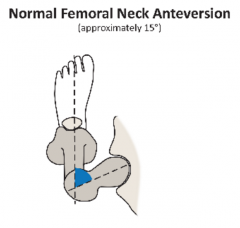
Normal: 10±7°
|
|
|
Name the 4 arteries supplying the femoral head. Which one is the major contributor? Where is the latter located? |
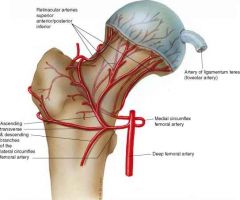
Medial femoral circumflex Lateral femoral circumflex Intramedullary supply (Artery of ligamentum teres – Insignificant) |
|
|
Define neck of femur and outline how # of the NOF can be classified based on their location and the impact on complication. |
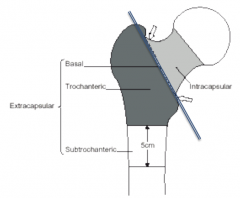
NOF – Up to 5cm inferior to the lesser trochanter In intracapsular #, blood supply to the capsule is at risk. |
|

|
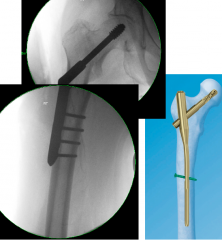
Dynamic hip screw |
|

|
Intramedullary nail |
|

|
Hemiprosthesis |
|

|
Total hip replacement |
|

|
Cannulated screw fixation |
|
|
Treatment options for extracapsular fracture of the hip. How do we decide which to use? |
Blood supply maintained ⟹ Preserve neck and head of femur Intramedullary nail – If DHS unstable (torque in IMN is lower because the axis is not offset) |
|
|
Outline Garden's classification of intracapsular fracture of the hip. What is the impact on blood supply? |

|
|
|
How would you treat Garden 4 intracapsular fractures in an otherwise healthy 19 year old? in a 91 year old? |
19 – Repair (40% failure rate that will require a likely tolerated second operation) 91 – Replace (90% failure rate of repair would require a likely non-tolerated second operation) |
|
|
T/F: Hip surgery in elderly with hip fracture may be delayed by a few days/weeks to increase the chance of a tolerated operation following trauma. |
False: Benefits of early mobilisation cannot be overemphasised. Operate as soon as possible. |
|
|
Surgical options for intracapsular hip fractures and which would you choose in the following scenarios: 1) Young (< 60) active patient 2) Active independent elderly 3) Non-active or dependent elderly |
3 Screw fixation – Young active Dynamic hip screw – Young active Hemiprosthesis – Non-active/Dependent Elder Total hip replacement – Active independent elder |
|
|
Which operation(s) for hip # may cause leg length discrepancy? |
THR |
|
|
Which operation(s) for hip # may cause non-union? |
Screws (varus malreduction) |
|

Describe and name the cause |
Shorten and externally rotated leg ⟹ Fracture of neck of femur |
|
|
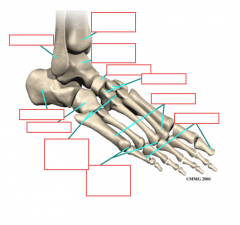
What articulation enables foot dorsiflexion and plantar flexion? |
Tibia-Talus |
|
|

|
|
|
Name 6 important ligaments in the stability of the ankle (and their insertions) |
Medial Deltoid – Medial malleolus to talus Lateral Calcaneofibular – Lateral malleolus to calcaneus Talofibular – Lateral malleolus to talus Tibia to fibula Syndesmosis of tibia and fibula – This is different from interrosseous membrane which runs along the entire length Anterior inferior tibiofibular Posterior tibiofibular |
|
|
What should you never forget on examination of the ankle (2)? |
Examine medial side Examine proximal fibula (Maisonneuve #) |
|
|
What is a syndesmosis? Why is it relevant in ankle? |
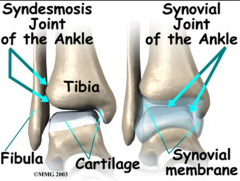
An immovable joint in which bones are joined by connective tissue (e.g. between the fibula and tibia at the ankle) |
|
|
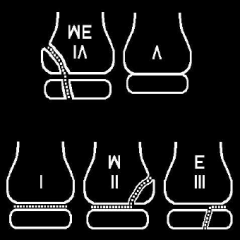
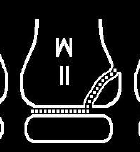
How are ankle fracture typically classified? |
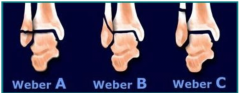
Weber classification (based on level of fibula #) Weber A – # distal to syndesmosis Weber B – # at syndesmosis Weber C – # above syndesmosis |
|
|
Emergency management of ankle fracture (3) |
Rebax 1) Reduce 2) Backslab (cast with moulding) to correct talar shift 3) Xray |
|
|
One absolute and 3 relative indications for surgery in ankle injury |
Absolute – Open injury Relative – Unstable fracture, Displacement, Talar shift |
|
|
Most common operation fix for ankle fracture. Name 4 other operations that can be used. |
Plates and screws Nails (calcaneus, talus, tibia or fibula) Syndesmosis sutures External: Ring fixator Mono-lateral frame ("ex-fix") |
|
|
Why is it important to examine the proximal fibula in ankle injury? |
Weber C fracture can present with proximal fibula fracture (Maisonneuve #) If tender around the area, X-ray If non-tender, report it in the notes (sue-protection) |
|
|
What is a Maisonneuve fracture? |
Spiral # of the proximal third of the fibula associated with a tear of the distal tibiofibular syndesmosis and the interosseous membrane. Associated with medial malleolus # or rupture of the deep deltoid ligament |
|
|
Treatment of Maisonneuve # (4) |
Rebax + Referral 1) Reduce 3) Backslab cast with moulding to correct talar shift 3) X-ray 4) Refer to ortho for syndesmosis screws |
|

What is wrong with this X-ray? |
Always reduce ankle fractures first (this X-ray should never have been acquired) |
|
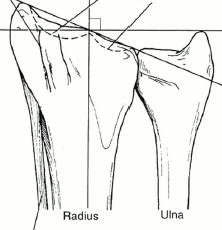
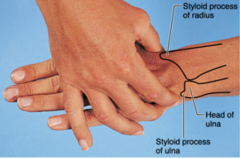
Name of the two grooves |
|
|
Name of the surface at which the ulna and radius articulate |
Sigmoid notch |
|

|
|
|
|
What do volar refer to? |
Synonym of palmar in hand |
|
|
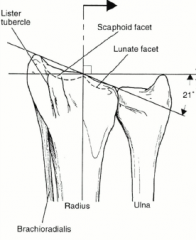
Normal angles of radius to interpret X-ray |
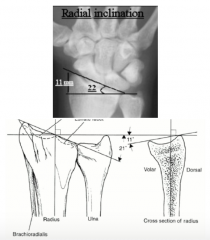
Rule of 11 11° of volar tilt 11mm of dradial offset 22° of radial inclination |
|

Characterise this fracture (3) and name one situation in which it occurs |
Dorsally angulated (dinner fork deformity) Dorsal displacement
Note: Colles' fracture in osteoporosis presents like that |
|

Characterise this fracture (3) and name one situation in which it occurs |
Volarly angulated Volarly displaced Extra-articular Situation – Falling on flexed wrist Note: Smiths' fracture presents like that |
|

Characterise this fracture (3) and name one situation in which it occurs |
Volarly displaced Extends into radiocarpal joint Situation – Fall on flexed wrist |
|
|
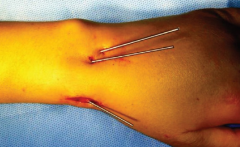
One non-surgical and 4 surgical management option of wrist fracture |
Non-surgical POP Surgical Manipulation under anaesthesia + POP Manipulation under anaesthesia + Percutaneous K wires Plates External fixation |
|
|
Percutaneous K wires |
|
|
1) How would you decide to operate on a wrist fracture? 2) How would you decide on which surgical management to choose from in a wrist #)? |
1) Difficult decision based on: - Severity (articular involvement?) - Patient's characteristics 2) K-wires as effective as plates but much cheaper (Drafft trial) |
|
|
Number of cervical, thoracic and lumbar vertebrae |
7C 12T 5L |
|
|
Specific early management (3) of spine in trauma (and how it integrates with the classical ABCDE) |
C spine triple immobilisation (during A of ABCD) ASIA chart for neuro exam during D Log-roll after ABCDE to look for ◾︎ Penetrating injuries ◾︎ Spinal process tenderness ◾︎ Asymmetry ◾︎ PR (tone, sensation and squeeze) |
|
|
What imaging is used as part of the primary survey in ATLS? What if spinal injury is suspected? |
CT If spinal injury suspected and neurological deficit, then MRI as well. |
|
|
What is the first vertebra that we can clearly see on a lateral X-ray of the spine |
C1 |
|
|
What is the first vertebra that we can clearly see on an AP X-ray of the spine |
C3 |
|
|
How can we see C1 in an AP film? |
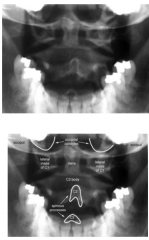
Through the mouth with mouth open |
|
|
How do you clinically rule out C spine injury? |
If all of A-F, then assess G-J and if they are all positive then cervical spine is cleared A) Patient fully alert and oriented. B) No head injury C) No drugs or alcohol D) No neck pain E) No abnormal neurology F) No distracting injury In the neck G) No bruising H) No deformity I) No tenderness J) Pain-free range of active movements |
|
|
How do you clinically rule out T and L spine injury? |
A+B+C A) Cooperative patient B) Non tender on log roll C) No tenderness at rest |
|
|
Some percentages. What fraction of trauma patients have spine fractures? Which of those have C spine fracture? Where do most of the latter occur (1st and 2nd most likely location)? |
4% of all trauma patients 55% in C spine 55% at C5/6, 20% at C1/2 |
|
|
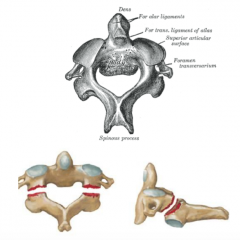
What is the atlas in relation to spine? |
C1 |
|
|
What fracture are patients diving in shallow water at risk of (2)? |
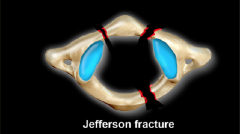
Jefferson fracture – Burst at C1 due to axial loading Flexion tear drop fracture |
|
|
What is Jefferson fracture? Mechanism? Example of a cause? |
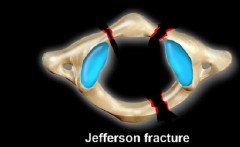
Burst fracture of C1 caused bydirect axial loading, eg diving into shallow water |
|
|
What is the axis in relation to spine? |
C2 |
|
|
What are C1 and C2 also called? |
C1 – Atlas C2 – Axis |
|
|
Most common fracture of C2? Name another fracture occurring at C2 and its mechanism. |
Odontoid process # = Peg # = Dens # Hangman's fracture (Picture below) Lateral part of C2 in the pars interarticularis Mechanism: hyperextension |
|
|
What does subluxation mean? |
Partial dislocation |
|

A patient underwent flexion distraction injury and rapidly develops neurology. X-ray is displayed. Likely diagnosis? |

Unifacet dislocation/subluxation (one vertebra dislocating anteriorly to its inferior neighbor) Unifacet demonstrates < 50% displacement while bifacet demonstrates > 50% displacement |
|

Diagnosis |
Bilateral facet dislocation (> 50% displacement of vertebra) |
|

|
Bilateral facet dislocation (> 50% displacement of vertebra) |
|
|
Why is the difference between bilateral and unilateral facet dislocation clinically relevant? |
Bilateral ⟹ High risk of cord injury |
|

Diagnosis, likely mechanism and prognosis |
Spinous process fracture (aka clay shoveler's fracture) |
|

Diagnosis, most likely location, likely mechanism, and possible structure at risk of damage |
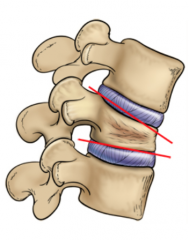
Compression wedge fracture C4-C6 Flexion and compression Posterior longitudinal ligament may rupture. |
|
|
What is clay shoveler's fracture? |

Spinous process fracture |
|
|
Coup du lapin in English |
Whiplash |
|
|
Most severe injury of the C spine. Mechanism of injury |
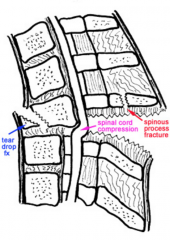
Flexion teardrop fracture Violent flexion and compression (eg diving head first, car collisions) |
|
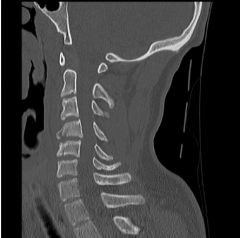
|
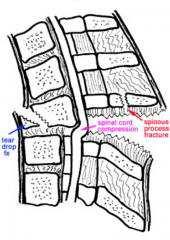
Flexion teardrop fracture |
|
|
What is peculiar about patients with ankylosing spondylitis when it comes to trauma? |
Don't immobilise as a normal C spine as the fused bones may break. |
|
|
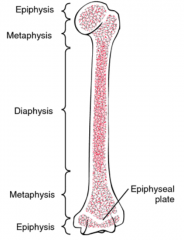
Difference between adults and children skeleton and its clinical significance |
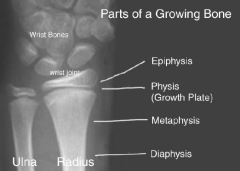
Physis (growth plate) between the metaphysis and epiphysis This is where most fractures occur |
|
|
What is the periosteum? |
Dense layer of vascular connective tissue enveloping the bones except at the surfaces of the joints |
|
|
T/F: the periosteum in the paediatric skeleton is thinner |
False: it is thicker |
|
T/F: the treatment of this # in a 6 year old is plating. |

False: remodelling is very effective |
|
|
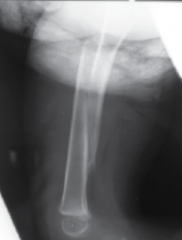
Name two fracture morphologies that occurs only in children |

Torus following axial compression due to viscoelasticity of the bone Greenstick (displayed) |
|

Diagnosis and likely mechanism of injury |
Torus fracture due to axial compression |
|
|
How can we perform a neurological assessment of an injury in a toddler? |
Sensation Autonomic – Rub pen along the skin. If it slides easily, then the skin is dry and is not sweating |
|
|
What classification do you know of that helps make a prognosis of epiphyseal fractures? |
Salter-Harris classification (higher means worse) |
|
|
Draw the metaphysis, physis and epiphysis of a generic bone and outline the fracture morphology in each class of the Salter-Harris classification |
SALTR Slipped (I) Above the physis (II) Lower than the physis (III) Through the physis (IV) Rammed together (V) |
|
|
Most common morphology of epiphyseal fracture in children? |
Salter-Harris II (75% of all) |
|

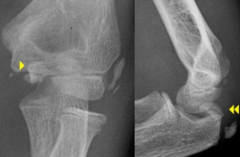
Salter-Harris class? |
Lower than the physis (when looked upside down) ⟹ SH III SALTR |
|

Salter-Harris class? |

Rammed together (tibial physis narrowed see bubble) ⟹ SH V SALTR |
|

Salter-Harris class? |
Slipped ⟹ SH I SALTR |
|

Salter-Harris class? |
Above the physis (when looked upside down) ⟹ SH II SALTR |
|

Salter-Harris class? |
Through the physis ⟹ SH IV SALTR |
|

What is depicted and what is a possible cause? |
Lateral displacement of the carpus towards the radius due to growth arrest of the radius. |
|
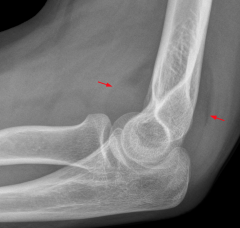
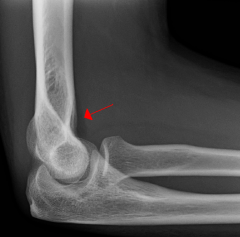
What do you see? What is the cause? |
Fat pad sign X-ray sign of an otherwise hidden fracture, caused by inflammation around the synovial membrane pushing the fat pads away from the bone (the pattern is therefore Grey ➙ Fat ➙ Grey ➙ Bone) |
|
What do you see? What is the cause? |
Normal anterior fat pad, not displaced (Grey ➙ Fat ➙ Bone rather than Grey ➙ Fat ➙ Grey ➙ Bone) |
|
|
T/F: a posterior fat pad on lateral XR of elbow is always abnormal |
True (even if it doesn't appear displaced) |
|
|
T/F: an anterior fat pad on lateral XR of elbow is always abnormal |
False |
|
|
Most likely cause of posterior fat pad sign in a child? adult? |
Child – Condylar fracture of the hymerus Adult – Radial head fracture |
|

8 year old. Diagnosis, likely mechanism and possible complications (2) |
Supracondylar fracture FOOSH from height Complication: Brachial artery tear and compartment syndrome Median nerve injury Radial nerve injury |
|
|
T/F: supracondylar fracture may appear subtle on XR (only as posterior fat pad sign) but then its prognosis is better. |

True: this is Gartland class 1 and confers better prognosis while the obvious displacement (displayed) is Gartland class 3 and has high risk of NV damage requiring urgent surgery |
|
|
T/F: Lateral mass/condyle fracture has a better prognosis than supracondylar fracture |
False: it is usually worse ans is a "not-to-miss" fracture of the elbow in children |
|
|
Name 3 fractures of the elbow that may occur in children |
Supracondylar fracture Lateral mass fracture (= lateral condyle fracture) Medial epicondyle fracture |
|

|

Lateral mass # (= lateral condyle #) |
|
|
Likely mechanism of lateral mass # |
FOOSH |
|

What is it and why is it challenging to diagnose? |
Medial epicondyle fracture Difficult because the broken epicondyle resembles a centre of ossification ⟹ It is essential to know the order of ossification centres (when they appear) |
|
|
Name the 6 ossification centres in the elbow and the age at which they appear |

CRITOE Capitellum – 1y Radial head – 3y Internal (medial) epicondyle – 5y Trochlear – 7y Olecranon – 9y External (lateral) epicondyle – 11y |
|
4 year old |
Medial epicondyle fracture (T appears at 7y) |
|

8 year old |
Trochlear ossification centre (T appears at 7y) |
|
|
A 46 year old man involved in a road traffic collision is found to have acute dyspnoea. Likely cause |
Posterior sternoclavicular joint dislocation ⟹ Clavicle pressed against mediastinum ⟹ Compression of trachea |
|
|
Name 3 possible signs and symptoms (besides injury) of posterior sternoclavicular joint dislocation |
Dyspnoea Dysphagia Paraesthesia of upper limb |
|

|
Posterior sternoclavicular joint dislocation |
|
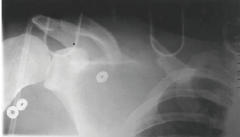
A patient presents with a swollen shoulder, pain and paraesthesia in the right arm as well as absent right radial and brachial pulses. He was sent to trauma following a road traffic collision. The X-ray is shown. State what you see on the X-ray and give the diagnosis. |
Scapulothoracic dissociation Laterally displaced scapula (edge of scapula displaced by > 1cm from spinous process compared to other side) |
|
|
NV complications of scapulothoracic dissociation (4) |
Nervous Brachial plexus Axillary nerve Vascular Subclavian artery Compound Flail upper limb (complete loss of sensory and motor functions) |
|
|
What artery is most likely involved in scapulothoracic dissociation? |
Subclavian |
|
|
Bases of treatment of scapulothoracic dissociations |
NV repair ± ORIF (open reduction internal fixation) |
|
|
PC A 34 year old complains of persistent pain in the midfoot. PMH Unremarkable apart from a bad fall from a tree on that foot when he was 32 (XR was unremarkable then). O/E Deformity Name and describe a possible cause. |

Lisfranc injury Tarsometatarsal fracture-dislocation often missed. |
|
|
Outline the management of Lisfranc fracture |
No weight bearing for 8/52 (cast) ORIF + Non-weight bearing for 3/52 |
|
|
Outline the scaphoid structure based on areas. Which area is most likely fracture? |
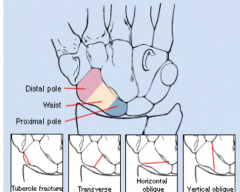
Waist is most likely to fracture (65%) |
|
|
Main worry in scaphoid fracture. What is the biggest RF for it in scaphoid fracture? |
Avascular necrosis More likely if # more proximal (due to retrograde blood flow) |
|
|
Most common mechanism of scaphoid fracture and one example where it occurs |
Axial load across hyper-extended and radially deviated wrist Example: contact sports |
|
|
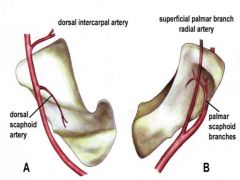
Blood supply to scaphoid |
|
|
|
4 clinical signs of scaphoid fracture |
Snuffbox tenderness dorsally Scaphoid tubercle tenderness volarly Pain with resisted pronation Pain when thumb is loaded axially |
|
|
Imaging in suspected scaphoid fracture |
X ray scaphoid view (30° wrist extension, 20° ulnar deviation) If negative and high level of suspicion, repeat X ray after 2/52 |
|
|
Treatment of scaphoid fracture (3) |
Cast Stable, non-displaced or no X-ray sign but high level of suspicion Unstable Bone graf If non union |
|
|
What does ATLS stand for? |
Advanced Trauma Life Support |
|
|
Define distracting injury |
Another injury which may 'distract' the patient from complaining about a possible spinal injury |